Department of Medicine, Division of Cardiovascular Medicine, Vanderbilt University Medical Center, Nashville, Tennessee.
Department of Biostatistics, Vanderbilt University Medical Center, Nashville, Tennessee.
JAMA Cardiol. 2022 Jul 1;7(7):733-741. doi: 10.1001/jamacardio.2022.0810.
Patients with early-onset atrial fibrillation (AF) are enriched for rare variants in cardiomyopathy and arrhythmia genes. The clinical significance of these rare variants in patients with early-onset AF is unknown.
To assess the association between rare variants in cardiomyopathy and arrhythmia genes detected in patients with early-onset AF and time to death.
DESIGN, SETTING, AND PARTICIPANTS: This prospective cohort study included participants with AF diagnosed before 66 years of age who underwent whole-genome sequencing through the National Heart, Lung and Blood Institute's Trans-Omics for Precision Medicine program. Participants were enrolled from November 23, 1999, to June 2, 2015. Data were analyzed from February 26 to September 19, 2021.
Rare variants identified in a panel of 145 genes that are included in cardiomyopathy and arrhythmia panels used by commercial clinical genetic testing laboratories.
The primary study outcome was time to death and was adjudicated from medical records and the National Death Index. Multivariable Cox proportional hazards regression was used to evaluate the association of disease-associated variants with risk of death after adjustment for age at AF diagnosis, sex, race, body mass index, left ventricular ejection fraction, and an interaction term of age at AF diagnosis and disease-associated variant status.
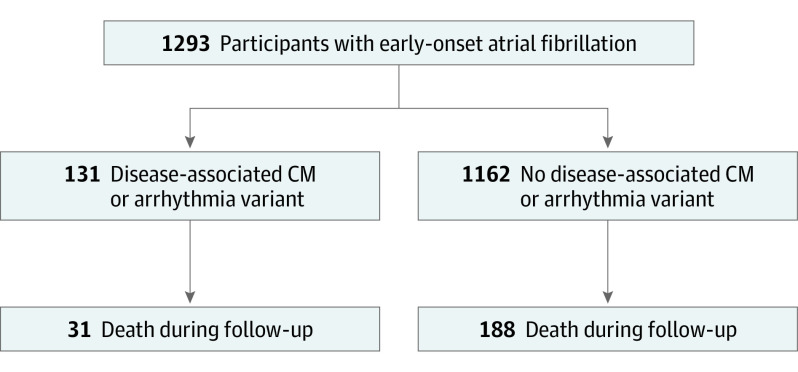
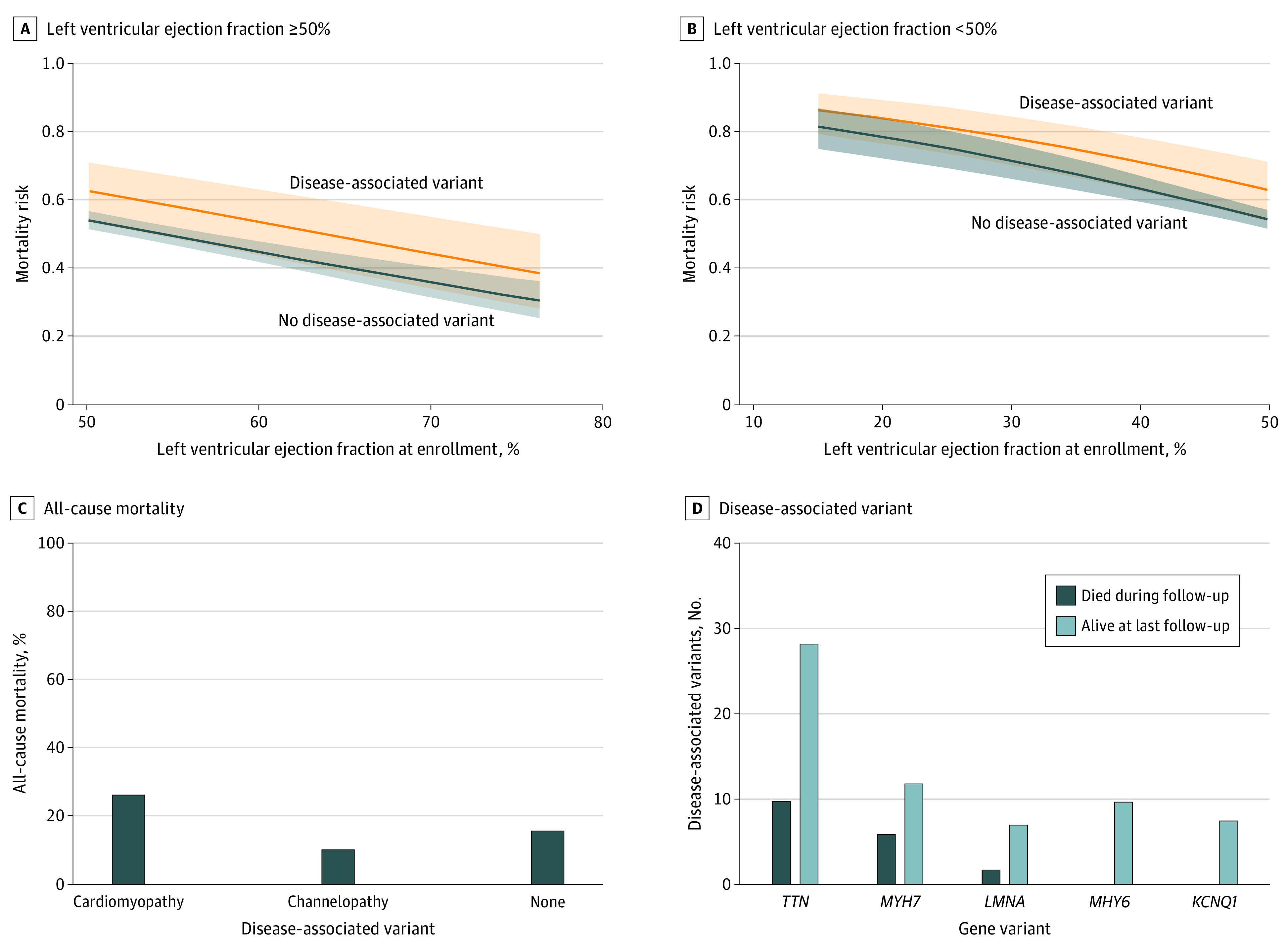
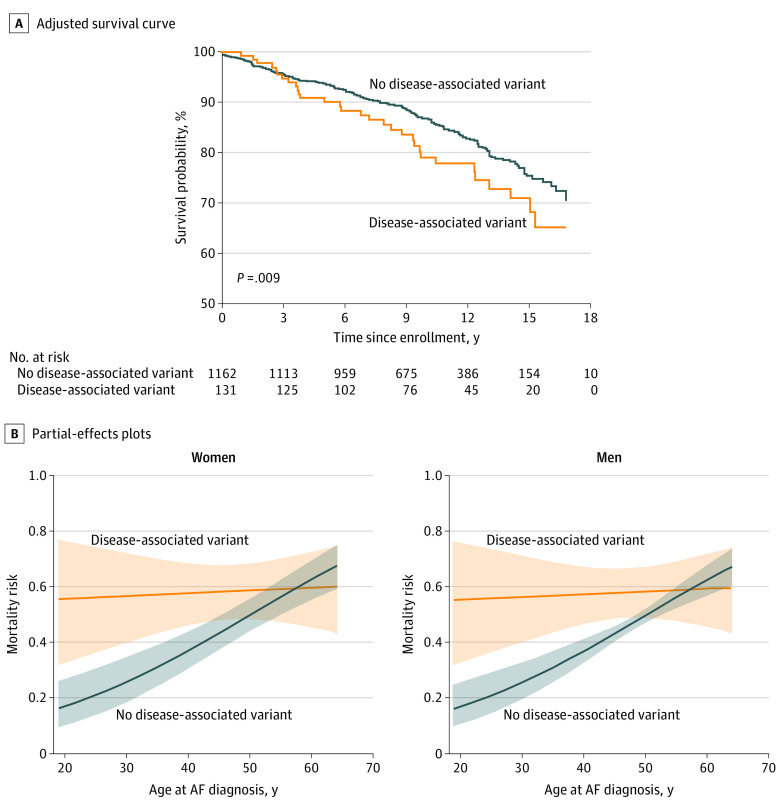
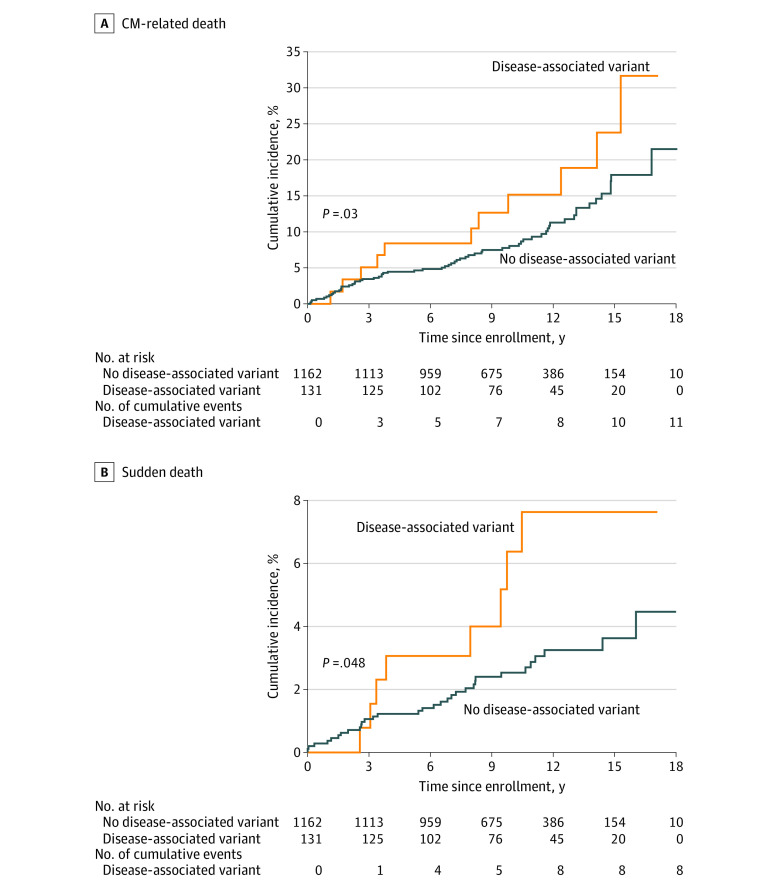
Among 1293 participants (934 [72%] male; median age at enrollment, 56.0 years; IQR, 48.0-61.0 years), disease-associated (pathogenic or likely pathogenic) rare variants were found in 131 (10%). During a median follow-up of 9.9 years (IQR, 6.9-13.2 years), 219 participants (17%) died. In univariable analysis, disease-associated variants were associated with an increased risk of mortality (hazard ratio, [HR], 1.5; 95% CI, 1.0-2.1; P = .05); the association remained significant in multivariable modeling when adjusted for age at AF diagnosis, sex, race, body mass index, left ventricular ejection fraction, and an interaction term between disease-associated variant status and age at AF diagnosis. The interaction demonstrated that disease-associated variants were associated with a significantly higher risk of mortality compared with no disease-associated variant when AF was diagnosed at a younger age (P = .008 for interaction). Higher body mass index (per IQR: HR, 1.4; 95% CI, 1.2-1.6; P < .001) and lower left ventricular ejection fraction (per IQR: HR, 0.8; 95% CI, 0.7-0.8; P < .001) were associated with higher mortality risk. There were 73 cardiomyopathy-related deaths, 40 sudden deaths, and 10 stroke-related deaths. Mortality among patients with the most prevalent genes with disease-associated variants was 26% (10 of 38 patients) for TTN, 33% (6 of 18) for MYH7, 22% (2 of 9) for LMNA, 0% (0 of 10) for MYH6, and 0% (0 of 8) for KCNQ1.
The findings suggest that rare variants in cardiomyopathy and arrhythmia genes may be associated with increased risk of mortality among patients with early-onset AF, especially those diagnosed at a younger age. Genetic testing may provide important prognostic information for patients with early-onset AF.
患有早发性心房颤动 (AF) 的患者在心肌病和心律失常基因中存在丰富的罕见变异。这些早发性 AF 患者中罕见变异的临床意义尚不清楚。
评估在早发性 AF 患者中检测到的心肌病和心律失常基因中的罕见变异与死亡时间之间的关联。
设计、地点和参与者:这项前瞻性队列研究纳入了通过国家心肺血液研究所的跨组学精准医学计划进行全基因组测序的诊断年龄在 66 岁以下的 AF 患者。参与者于 1999 年 11 月 23 日至 2015 年 6 月 2 日入组。数据于 2021 年 2 月 26 日至 9 月 19 日进行分析。
在商业临床遗传检测实验室使用的心肌病和心律失常面板中包含的 145 个基因的面板中鉴定出的罕见变异。
主要研究结果是死亡时间,并从病历和国家死亡指数中进行裁决。多变量 Cox 比例风险回归用于评估在调整 AF 诊断年龄、性别、种族、体重指数、左心室射血分数以及 AF 诊断和疾病相关变异状态的交互项后,疾病相关变异与死亡风险之间的关联。
在 1293 名参与者(934 名 [72%] 男性;中位入组年龄为 56.0 岁;IQR,48.0-61.0 岁)中,发现 131 名(10%)存在疾病相关(致病性或可能致病性)罕见变异。在中位随访 9.9 年(IQR,6.9-13.2 年)期间,219 名参与者(17%)死亡。在单变量分析中,疾病相关变异与死亡率增加相关(风险比 [HR],1.5;95%CI,1.0-2.1;P=0.05);在调整 AF 诊断年龄、性别、种族、体重指数、左心室射血分数以及疾病相关变异状态与 AF 诊断之间的交互项后,这种关联在多变量模型中仍然显著。交互作用表明,与没有疾病相关变异的情况相比,当 AF 更早诊断时,疾病相关变异与更高的死亡率风险显著相关(交互作用 P=0.008)。更高的体重指数(每 IQR:HR,1.4;95%CI,1.2-1.6;P<0.001)和更低的左心室射血分数(每 IQR:HR,0.8;95%CI,0.7-0.8;P<0.001)与更高的死亡率风险相关。共有 73 例心肌病相关死亡、40 例猝死和 10 例中风相关死亡。最常见的具有疾病相关变异的基因(TTN、MYH7、LMNA、MYH6 和 KCNQ1)患者的死亡率分别为 26%(38 例患者中的 10 例)、33%(18 例患者中的 6 例)、22%(9 例患者中的 2 例)、0%(10 例患者中的 0 例)和 0%(8 例患者中的 0 例)。
研究结果表明,心肌病和心律失常基因中的罕见变异可能与早发性 AF 患者的死亡率增加相关,尤其是那些更早诊断的患者。基因检测可能为早发性 AF 患者提供重要的预后信息。