Yeter Tuğçe, Onur Gönen Aybike, Türeci Ercan
Department of Anaesthesiology and Reanimation, Dr. Sadi Konuk Training and Research Hospital, İstanbul, Turkey.
Department of Anaesthesiology and Reanimation, İstanbul University Cerrahpaşa Faculty of Medicine, İstanbul, Turkey.
Turk J Anaesthesiol Reanim. 2022 Apr;50(2):114-120. doi: 10.5152/TJAR.2021.21217.
Electroconvulsive therapy is an effective non-pharmacological treatment for refractory mental illness, where a generalized seizure is induced under general anaesthesia. An ideal combination of the anaesthetic drugs should keep the patient paralyzed and unconscious for a few minutes, while allowing rapid recovery, supporting peri-procedural hemodynamic and respiratory stability, and permitting an effective treatment. We examined whether dexmedetomidine is advantageous over propofol as an adjunct to ketamine during electroconvulsive therapy.
Sixty patients were randomly assigned to receive either ketamine-propofol or ketamine-dexmedetomidine. Periprocedural hemodynamic and respiratory parameters, recovery metrics, seizure length, side effects, and cost of treatment were compared between the 2 groups.
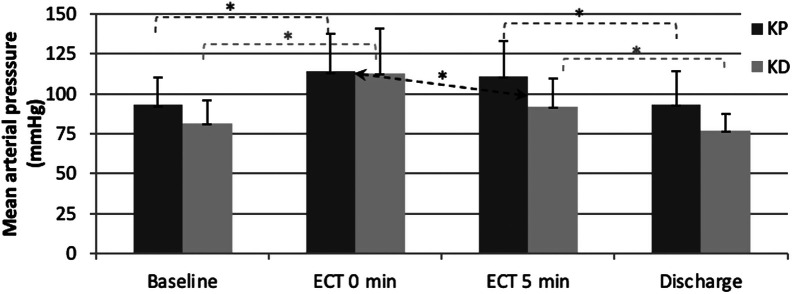
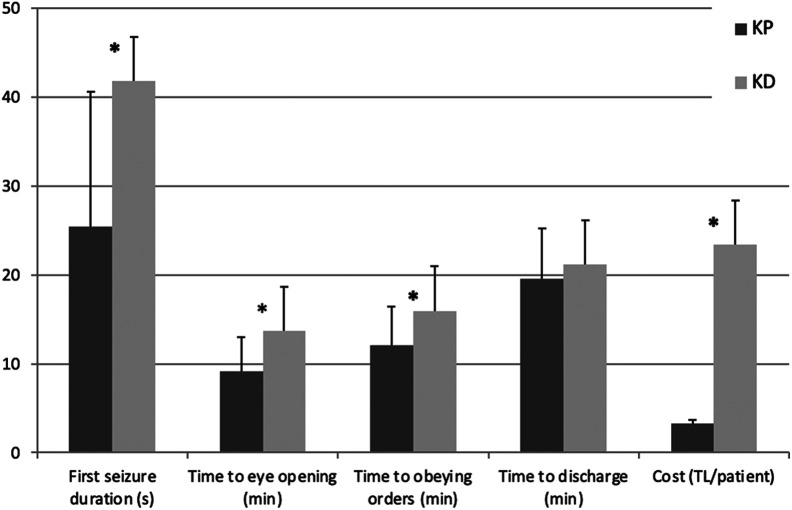
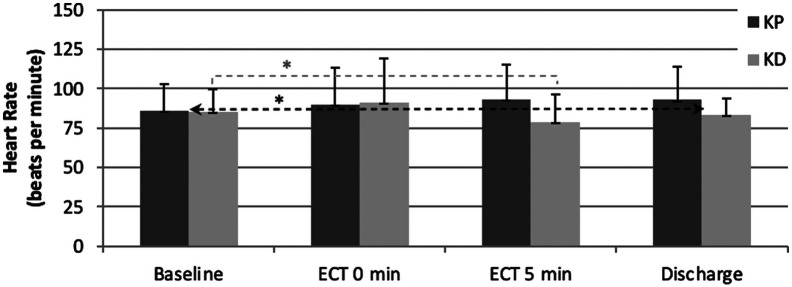
Hemodynamic response, respiratory status, and side effect profiles in ketamine-dexmedetomidine and ketamine-propofol groups were similar. Ketamine-dexmedetomidine combination showed a slight advantage with returning to baseline mean arterial pressure levels sooner. Seizures lasted longer in ketamine-dexmedetomidine group (41.8 seconds vs 25.4 seconds, P =.001). Recovery time was similar in 2 groups (P =.292); however, time to eye opening and following orders was longer in ketamine-dexmedetomidine (P < .001 and P =.003). The cost of treatment for ketamine-dexmedetomidine was much higher than ketamine-propofol (P < .001).
Ketamine-dexmedetomidine induction led to longer seizures during electroconvulsive therapy compared to ketamine-propofol. We observed slightly better hemodynamic stability with dexmedetomidine compared to propofol. Despite dexmedetomidine's disadvantages with a longer duration of administration, possible higher cost, and minor delay in initial recovery, it should be considered as a feasible agent for electroconvulsive therapy anaesthesia.
电休克治疗是一种治疗难治性精神疾病的有效非药物疗法,即在全身麻醉下诱发全身性癫痫发作。理想的麻醉药物组合应使患者在几分钟内保持麻痹和无意识状态,同时实现快速恢复,维持围手术期血流动力学和呼吸稳定性,并确保治疗有效。我们研究了在电休克治疗期间,右美托咪定作为氯胺酮辅助用药是否优于丙泊酚。
60例患者被随机分配接受氯胺酮 - 丙泊酚或氯胺酮 - 右美托咪定治疗。比较两组的围手术期血流动力学和呼吸参数、恢复指标、癫痫发作时长、副作用及治疗费用。
氯胺酮 - 右美托咪定组和氯胺酮 - 丙泊酚组的血流动力学反应、呼吸状态及副作用情况相似。氯胺酮 - 右美托咪定组合在更快恢复至基线平均动脉压水平方面略有优势。氯胺酮 - 右美托咪定组癫痫发作持续时间更长(41.8秒对25.4秒,P = 0.001)。两组恢复时间相似(P = 0.292);然而,氯胺酮 - 右美托咪定组睁眼和遵嘱时间更长(P < 0.001和P = 0.003)。氯胺酮 - 右美托咪定的治疗费用远高于氯胺酮 - 丙泊酚(P < 0.001)。
与氯胺酮 - 丙泊酚相比,氯胺酮 - 右美托咪定诱导在电休克治疗期间导致更长的癫痫发作。我们观察到与丙泊酚相比,右美托咪定的血流动力学稳定性略好。尽管右美托咪定存在给药时间长、可能费用更高以及初始恢复略有延迟等缺点,但它应被视为电休克治疗麻醉的一种可行药物。