Laville Solène M, Couturier Aymeric, Lambert Oriane, Metzger Marie, Mansencal Nicolas, Jacquelinet Christian, Laville Maurice, Frimat Luc, Fouque Denis, Combe Christian, Robinson Bruce M, Stengel Bénédicte, Liabeuf Sophie, Massy Ziad A
Department of Clinical Pharmacology, Amiens University Hospital, Amiens, France.
MP3CV Laboratory, EA7517, University of Picardie Jules Verne, Amiens, France.
Nephrol Dial Transplant. 2022 Feb 26;38(1):184-92. doi: 10.1093/ndt/gfac045.
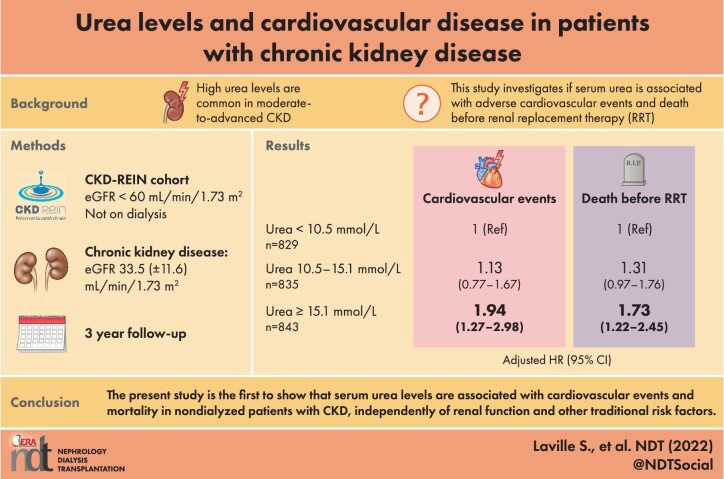
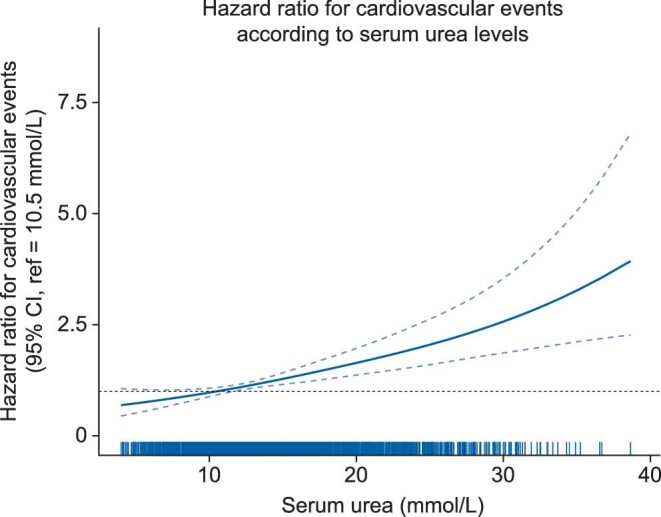
Elevated serum urea levels are common in moderate-to-advanced CKD. Several studies have shown that urea is a direct and indirect uremic toxin, especially with regard to cardiovascular disease. We sought to determine whether serum urea levels are associated with adverse cardiovascular events and death before renal replacement therapy (RRT) in patients with CKD.
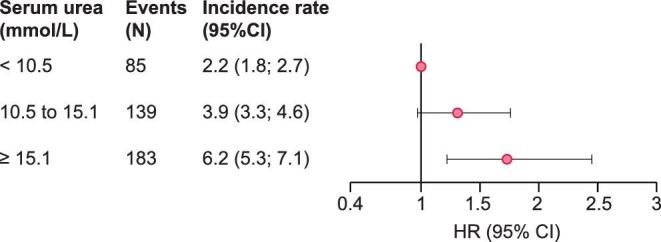
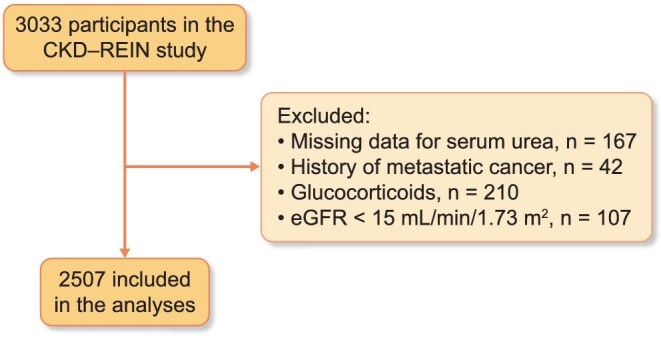
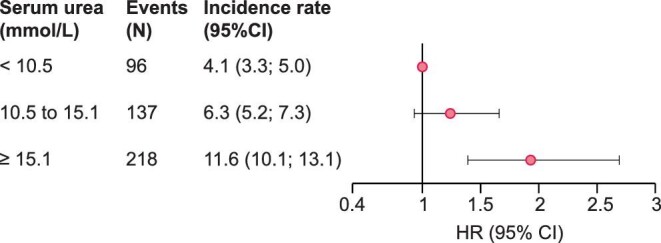
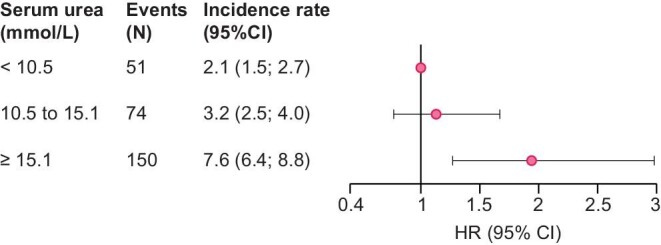
CKD-REIN is a prospective cohort of CKD nephrology outpatients not receiving maintenance dialysis. The 2507 patients included in the analysis were divided into three groups according to the baseline serum urea level (T1 < 10.5, T2:10.5 to 15.1, and T3 ≥ 15.1 mmol/L). Cox proportional hazard models were used to estimate hazard ratios (HRs) for first atheromatous or nonatheromatous cardiovascular (CV) events, and all-cause mortality before RRT. The models were adjusted for baseline comorbidities, laboratory data, and medications.
Of the 2507 included patients (median [interquartile range (IQR)] age: 69[61-77]; mean (standard deviation) eGFR 33.5(11.6) mL/min/1.73 m²), 54% had a history of cardiovascular disease. After multiple adjustments for cardiovascular risk factors (including eGFR), patients in T3 had a higher risk of atheromatous and nonatheromatous cardiovascular events than patient in T1 (n events = 451, HR[95%CI]: 1.93[1.39-2.69]). The adjusted HRs for death before RRT (n events = 407) were 1.31[0.97; 1.76] and 1.73[1.22; 2.45] for patients T2 and those in T3, respectively.
Our data suggested that urea is a predictor of cardiovascular outcomes beyond CV risk factors including eGFR.
血清尿素水平升高在中晚期慢性肾脏病(CKD)中很常见。多项研究表明,尿素是一种直接和间接的尿毒症毒素,尤其是在心血管疾病方面。我们试图确定血清尿素水平是否与CKD患者在肾脏替代治疗(RRT)前的不良心血管事件和死亡相关。
CKD-REIN是一个未接受维持性透析的CKD肾病门诊患者的前瞻性队列。纳入分析的2507例患者根据基线血清尿素水平分为三组(T1<10.5、T2:10.5至15.1、T3≥15.1 mmol/L)。采用Cox比例风险模型估计首次动脉粥样硬化或非动脉粥样硬化心血管(CV)事件以及RRT前全因死亡率的风险比(HR)。模型对基线合并症、实验室数据和药物进行了校正。
在纳入的2507例患者中(年龄中位数[四分位间距(IQR)]:69[61-77];平均(标准差)估算肾小球滤过率(eGFR)33.5(11.6)mL/min/1.73 m²),54%有心血管疾病史。在对心血管危险因素(包括eGFR)进行多次校正后,T3组患者发生动脉粥样硬化和非动脉粥样硬化心血管事件的风险高于T1组患者(事件数n = 451,HR[95%CI]:1.93[1.39-2.69])。T2组和T3组患者RRT前死亡的校正HR分别为1.31[0.97;1.76]和1.73[1.22;2.45]。
我们的数据表明,除了包括eGFR在内的心血管危险因素外,尿素是心血管结局的一个预测指标。