Guan Yaping, Feng Dongfeng, Yin Beibei, Li Kun, Wang Jun
Department of Oncology, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Jinan, China Shandong Lung Cancer Institute, Jinan, China.
Department of PET/CT, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Jinan, China.
Ther Adv Med Oncol. 2022 May 6;14:17588359221096877. doi: 10.1177/17588359221096877. eCollection 2022.
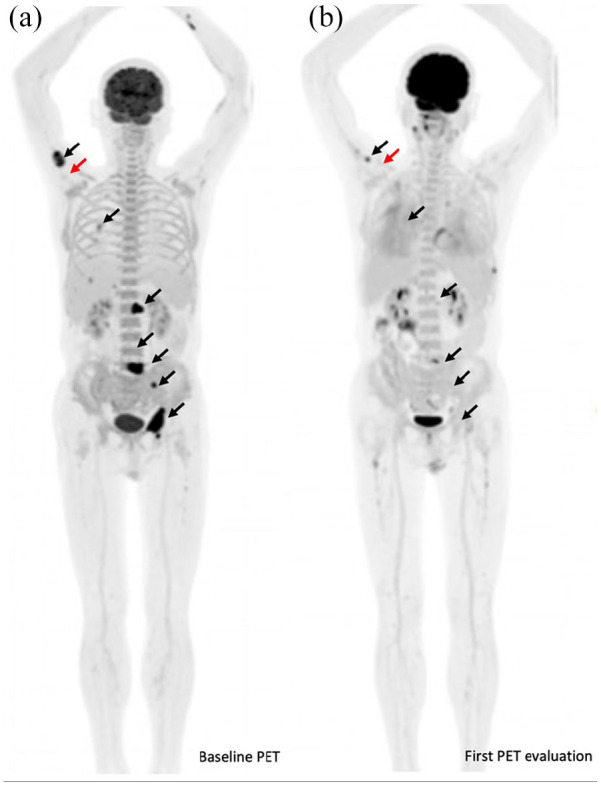
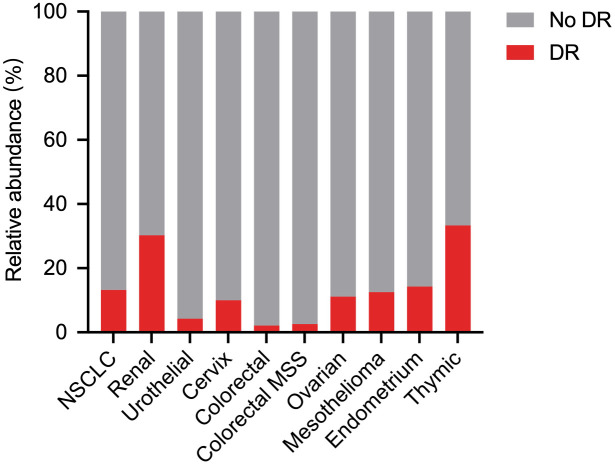
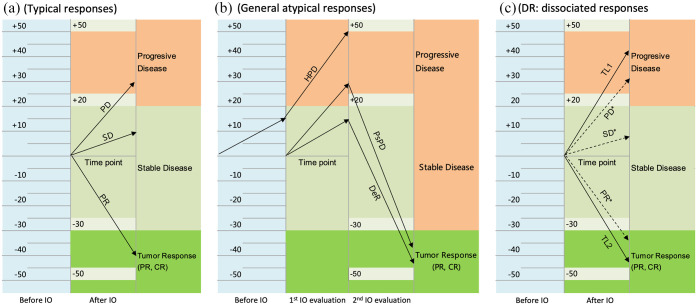
Immune checkpoint blockade using immune checkpoint inhibitors, including cytotoxic T-lymphocyte-associated antigen-4 and programmed cell death protein-1/programmed cell death ligand-1 inhibitors, has revolutionized systematic treatment for advanced solid tumors, with unprecedented survival benefit and tolerable toxicity. Nivolumab, pembrolizumab, cemiplimab, avelumab, durvalumab, atezolizumab, and ipilimumab are currently approved standard treatment options for various human cancer types. The response rate to immune checkpoint inhibitors, however, is unsatisfactory, and unexpectedly, atypical radiological responses, including delayed responses, pseudoprogression, hyperprogression, and dissociated responses (DRs), are observed in a small subgroup of patients. The benefit of immunotherapy for advanced patients who exhibit atypical responses is underestimated according to the conventional response evaluation criteria in solid tumors (RECIST). In particular, DR is considered a mixed radiological or heterogeneous response pattern when responding and nonresponding lesions or new lesions coexist simultaneously. The rate of DR reported in different studies encompass a wide range of 3.3-47.8% based on diverse definition of DR. Although DR is also associated with treatment efficacy and a favorable prognosis, it is different from pseudoprogression, which has concordant progressive lesions and can be regularly captured by immune RECIST. This review article aims to comprehensively determine the frequency, definition, radiological evaluation, probable molecular mechanisms, prognosis, and clinical management of immune-related DR and help clinicians and radiologists objectively and correctly interpret this specific atypical response and better understand and manage cancer patients with immunotherapy and guarantee their best clinical benefit.
使用免疫检查点抑制剂进行免疫检查点阻断,包括细胞毒性T淋巴细胞相关抗原4和程序性细胞死亡蛋白1/程序性细胞死亡配体1抑制剂,已经彻底改变了晚期实体瘤的系统治疗,带来了前所未有的生存获益且毒性可耐受。纳武利尤单抗、帕博利珠单抗、西米普利单抗、阿维鲁单抗、度伐利尤单抗、阿替利珠单抗和伊匹木单抗目前是针对各种人类癌症类型批准的标准治疗选择。然而,免疫检查点抑制剂的缓解率并不理想,而且出乎意料的是,在一小部分患者中观察到了非典型放射学反应,包括延迟反应、假性进展、超进展和分离反应(DRs)。根据实体瘤的传统反应评估标准(RECIST),免疫疗法对表现出非典型反应的晚期患者的益处被低估了。特别是,当反应性和非反应性病变或新病变同时共存时,DR被认为是一种混合放射学或异质性反应模式。基于对DR的不同定义,不同研究报道的DR发生率在3.3%-47.8%的广泛范围内。尽管DR也与治疗疗效和良好预后相关,但它与假性进展不同,假性进展具有一致的进展性病变,并且可以通过免疫RECIST定期捕获。这篇综述文章旨在全面确定免疫相关DR的频率、定义、放射学评估、可能的分子机制、预后和临床管理,帮助临床医生和放射科医生客观、正确地解释这种特定的非典型反应,更好地理解和管理接受免疫治疗的癌症患者,并确保他们获得最佳临床获益。