Golesworthy Bryn, Wang Yifan, Tanti Amanda, Pacis Alain, Romero Joan Miguel, Cuggia Adeline, Domecq Celine, Bourdel Guillaume, Denroche Robert E, Jang Gun Ho, Grant Robert C, Borgida Ayelet, Grünwald Barbara T, Dodd Anna, Wilson Julie M, Bourque Guillaume, O'Kane Grainne M, Fischer Sandra E, Kron Chelsea Maedler, Fiset Pierre-Olivier, Omeroglu Atilla, Foulkes William D, Gallinger Steven, Guiot Marie-Christine, Gao Zu-Hua, Zogopoulos George
The Research Institute of the McGill University Health Centre, Montreal, QC, Canada.
The Rosalind and Morris Goodman Cancer Institute of McGill University, Montreal, QC, Canada.
Front Oncol. 2022 Apr 25;12:860767. doi: 10.3389/fonc.2022.860767. eCollection 2022.
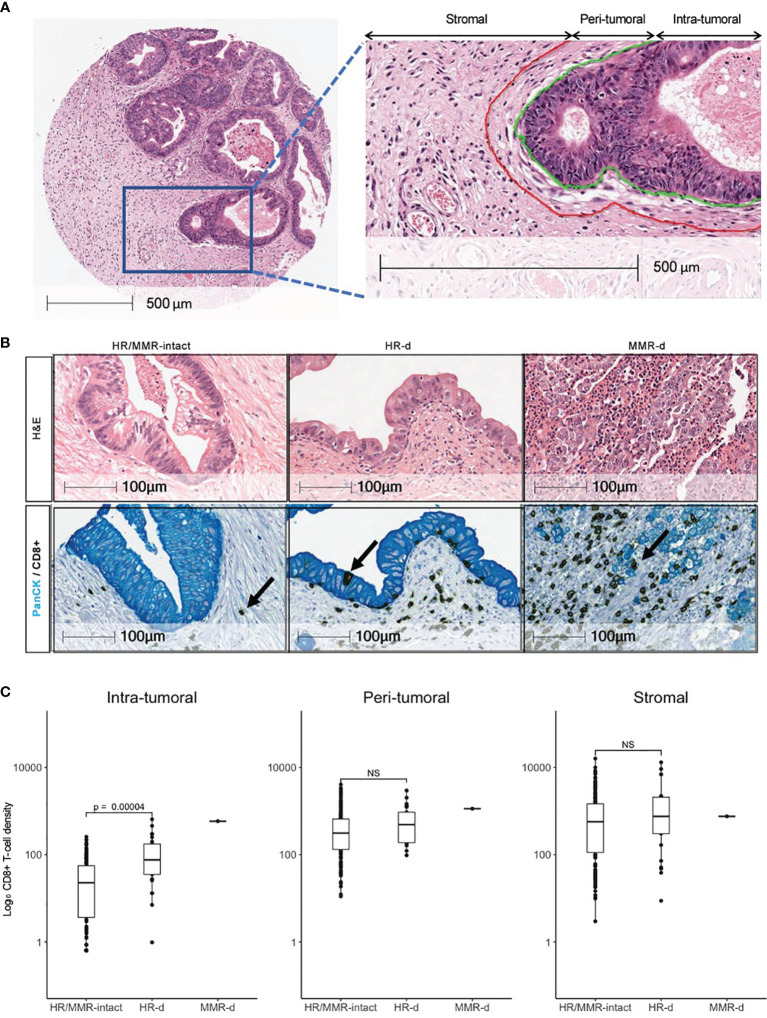
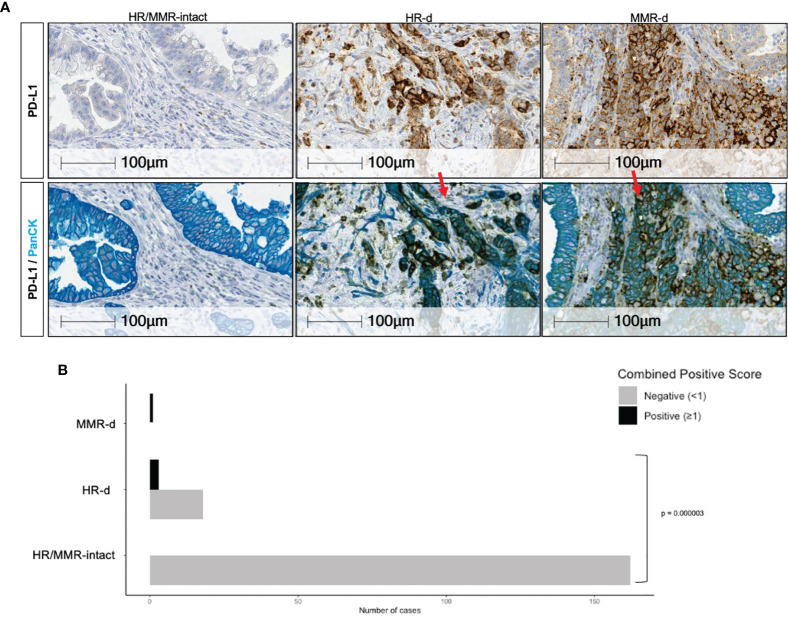
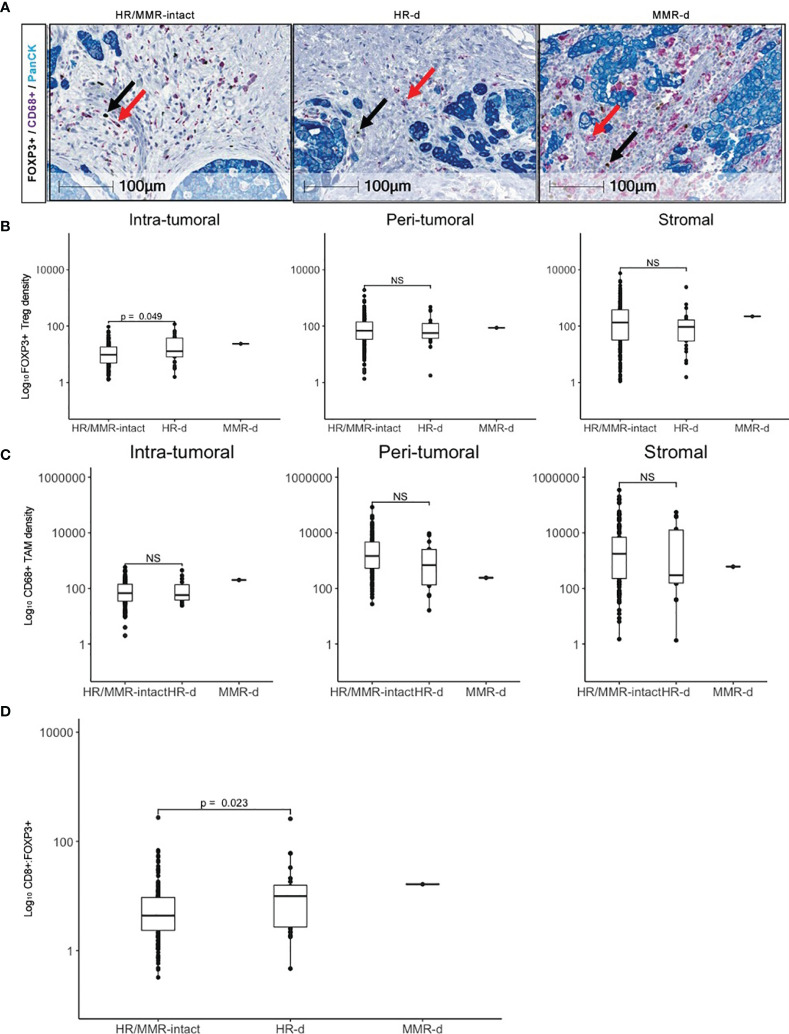
The immune contexture of pancreatic ductal adenocarcinoma (PDAC) is generally immunosuppressive. A role for immune checkpoint inhibitors (ICIs) in PDAC has only been demonstrated for the rare and hypermutated mismatch repair (MMR) deficient (MMR-d) subtype. Homologous recombination repair (HR) deficient (HR-d) PDAC is more prevalent and may encompass up to 20% of PDAC. Its genomic instability may promote a T-cell mediated anti-tumor response with therapeutic sensitivity to ICIs. To investigate the immunogenicity of HR-d PDAC, we used multiplex immunohistochemistry (IHC) to compare the density and spatial distribution of CD8+ cytotoxic T-cells, FOXP3+ regulatory T-cells (Tregs), and CD68+ tumor-associated macrophages (TAMs) in HR-d HR/MMR-intact PDAC. We also evaluated the IHC positivity of programmed death-ligand 1 (PD-L1) across the subgroups. 192 tumors were evaluated and classified as HR/MMR-intact (n=166), HR-d (n=25) or MMR-d (n=1) based on germline testing and tumor molecular hallmarks. Intra-tumoral CD8+ T-cell infiltration was higher in HR-d HR/MMR-intact PDAC (p<0.0001), while CD8+ T-cell densities in the peri-tumoral and stromal regions were similar in both groups. HR-d PDAC also displayed increased intra-tumoral FOXP3+ Tregs (p=0.049) and had a higher CD8+:FOXP3+ ratio (p=0.023). CD68+ TAM expression was similar in HR-d and HR/MMR-intact PDAC. Finally, 6 of the 25 HR-d cases showed a PD-L1 Combined Positive Score of >=1, whereas none of the HR/MMR-intact cases met this threshold (p<0.00001). These results provide immunohistochemical evidence for intra-tumoral CD8+ T-cell enrichment and PD-L1 positivity in HR-d PDAC, suggesting that HR-d PDAC may be amenable to ICI treatment strategies.
胰腺导管腺癌(PDAC)的免疫微环境通常具有免疫抑制作用。免疫检查点抑制剂(ICI)在PDAC中的作用仅在罕见的、高突变的错配修复(MMR)缺陷(MMR-d)亚型中得到证实。同源重组修复(HR)缺陷(HR-d)的PDAC更为常见,可能占PDAC的20%。其基因组不稳定性可能促进T细胞介导的抗肿瘤反应,并对ICI具有治疗敏感性。为了研究HR-d PDAC的免疫原性,我们使用多重免疫组织化学(IHC)比较了HR-d和HR/MMR完整的PDAC中CD8+细胞毒性T细胞、FOXP3+调节性T细胞(Tregs)和CD68+肿瘤相关巨噬细胞(TAM)的密度和空间分布。我们还评估了各亚组中程序性死亡配体1(PD-L1)的IHC阳性情况。根据种系检测和肿瘤分子特征,对192个肿瘤进行了评估,并分为HR/MMR完整组(n=166)、HR-d组(n=25)或MMR-d组(n=1)。HR-d组的肿瘤内CD8+T细胞浸润高于HR/MMR完整组(p<0.0001),而两组肿瘤周围和基质区域的CD8+T细胞密度相似。HR-d PDAC的肿瘤内FOXP3+Tregs也增加(p=0.049),且CD8+:FOXP3+比值更高(p=0.023)。HR-d组和HR/MMR完整组的CD68+TAM表达相似。最后,25例HR-d病例中有6例的PD-L1联合阳性评分>=1,而HR/MMR完整组中无一例达到该阈值(p<0.00001)。这些结果为HR-d PDAC中肿瘤内CD8+T细胞富集和PD-L1阳性提供了免疫组织化学证据,表明HR-d PDAC可能适合ICI治疗策略。