Library of Graduate School, Chinese People's Liberation Army General Hospital, Beijing, 100853, China.
Ping An Healthcare Technology, Beijing, China.
BMC Pulm Med. 2022 May 12;22(1):193. doi: 10.1186/s12890-022-01963-7.
Several studies have investigated the correlation between physiological parameters and the risk of acute respiratory distress syndrome (ARDS), in addition, etiology-associated heterogeneity in ARDS has become an emerging topic quite recently; however, the intersection between the two, which is early prediction of target conditions in etiology-specific ARDS, has not been well-studied. We aimed to develop and validate a machine-learning model for the early prediction of moderate-to-severe condition of inhalation-induced ARDS.
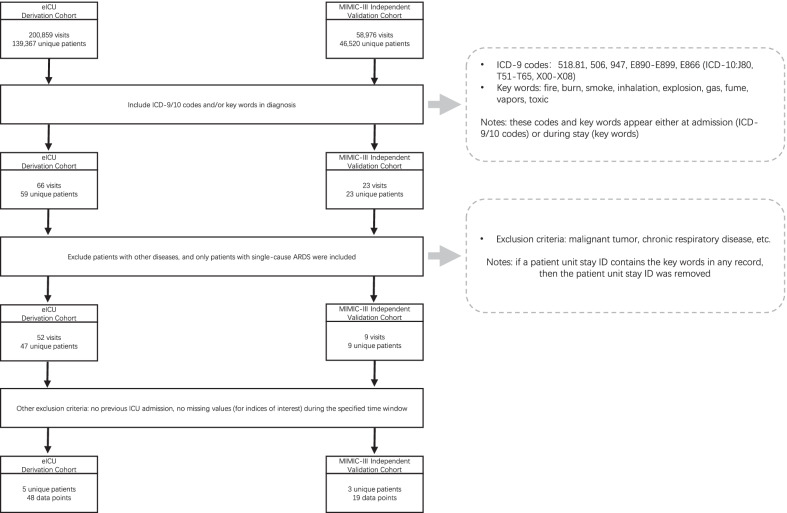
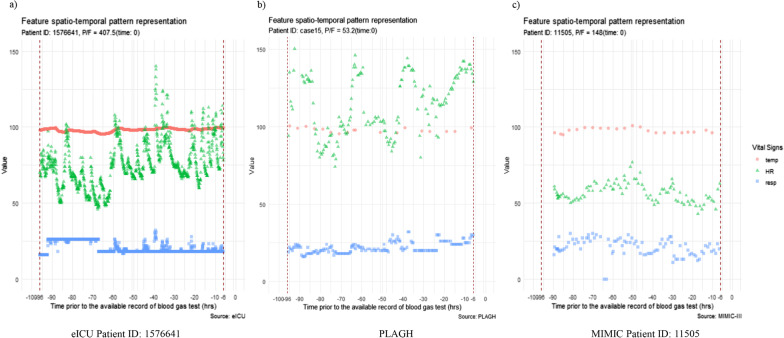
Clinical expertise was applied with data-driven analysis. Using data from electronic intensive care units (retrospective derivation cohort) and the three most accessible vital signs (i.e. heart rate, temperature, and respiratory rate) together with feature engineering, we applied a random forest approach during the time window of 90 h that ended 6 h prior to the onset of moderate-to-severe respiratory failure (the ratio of partial pressure of arterial oxygen to fraction of inspired oxygen ≤ 200 mmHg).
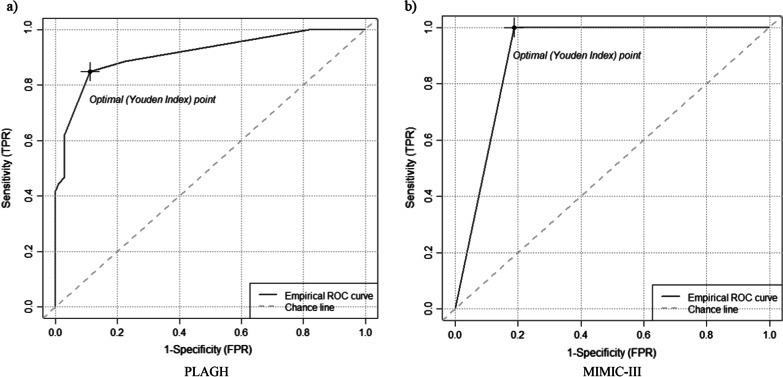
The trained random forest classifier was validated using two independent validation cohorts, with an area under the curve of 0.9127 (95% confidence interval 0.8713-0.9542) and 0.9026 (95% confidence interval 0.8075-1), respectively. A Stable and Interpretable RUle Set (SIRUS) was used to extract rules from the RF to provide guidelines for clinicians. We identified several predictive factors, including resp_96h_6h_min < 9, resp_96h_6h_mean ≥ 16.1, HR_96h_6h_mean ≥ 102, and temp_96h_6h_max > 100, that could be used for predicting inhalation-induced ARDS (moderate-to-severe condition) 6 h prior to onset in critical care units. ('xxx_96h_6h_min/mean/max': the minimum/mean/maximum values of the xxx vital sign collected during a 90 h time window beginning 96 h prior to the onset of ARDS and ending 6 h prior to the onset from every recorded blood gas test).
This newly established random forest‑based interpretable model shows good predictive ability for moderate-to-severe inhalation-induced ARDS and may assist clinicians in decision-making, as well as facilitate the enrolment of patients in prevention programmes to improve their outcomes.
多项研究调查了生理参数与急性呼吸窘迫综合征(ARDS)风险之间的相关性,此外,ARDS 的病因相关性异质性最近也成为一个新兴话题;然而,这两者之间的交集,即病因特异性 ARDS 中目标病症的早期预测,尚未得到很好的研究。我们旨在开发和验证一种用于预测吸入性 ARDS 中中重度疾病的机器学习模型。
采用临床专业知识和数据驱动分析。使用电子重症监护病房的数据(回顾性推导队列)和三个最易获得的生命体征(即心率、体温和呼吸率),以及特征工程,我们在 90 小时的时间窗口内应用随机森林方法,该时间窗口在中重度呼吸衰竭(动脉血氧分压与吸入氧分数之比≤200mmHg)发作前 6 小时结束。
使用两个独立的验证队列验证了训练好的随机森林分类器,其曲线下面积分别为 0.9127(95%置信区间 0.8713-0.9542)和 0.9026(95%置信区间 0.8075-1)。使用稳定且可解释的规则集(SIRUS)从 RF 中提取规则,为临床医生提供指导。我们确定了几个预测因素,包括 resp_96h_6h_min<9、resp_96h_6h_mean≥16.1、HR_96h_6h_mean≥102 和 temp_96h_6h_max>100,这些因素可用于预测重症监护病房中吸入性 ARDS(中重度疾病)在发病前 6 小时。('xxx_96h_6h_min/mean/max':ARDS 发作前 96 小时开始的 90 小时时间窗口内收集的 xxx 生命体征的最小值/平均值/最大值,在每个记录的血气检查中结束前 6 小时)。
这个新建立的基于随机森林的可解释模型对中重度吸入性 ARDS 具有良好的预测能力,可能有助于临床医生做出决策,并有助于将患者纳入预防计划以改善其结局。