Department of Intensive Care Medicine, Kameda Medical Center, Kamogawa, Japan.
Emergency and Trauma Center, Kameda Medical Center, Kamogawa, Chiba, 296-8602, Japan.
Crit Care. 2022 May 13;26(1):136. doi: 10.1186/s13054-022-04013-0.
Hospital- and community-onset sepsis are significant sepsis subgroups. Japanese data comparing these subgroups are limited. This study aimed to describe the epidemiology of hospital- and community-onset sepsis in critical care units in Japan.
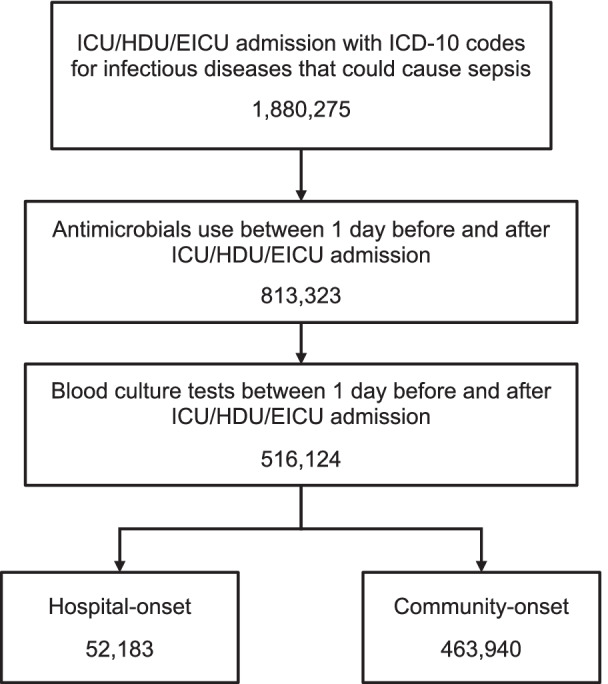
We performed a retrospective cohort study using the Japanese Diagnosis and Procedure Combination database. Adult patients admitted to critical care units with sepsis from April 2010 to March 2020 were included. Sepsis cases were identified based on ICD-10 codes for infectious diseases, procedure codes for blood culture tests, and medication codes for antimicrobials. Patients' characteristics, in-hospital mortality, and resource utilization were assessed. The in-hospital mortality between groups was compared using the Poisson regression generalized linear mixed-effect model.
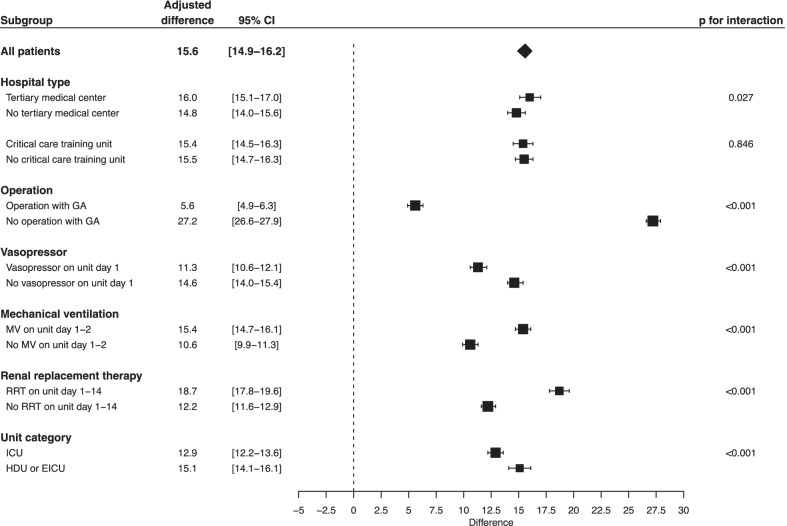
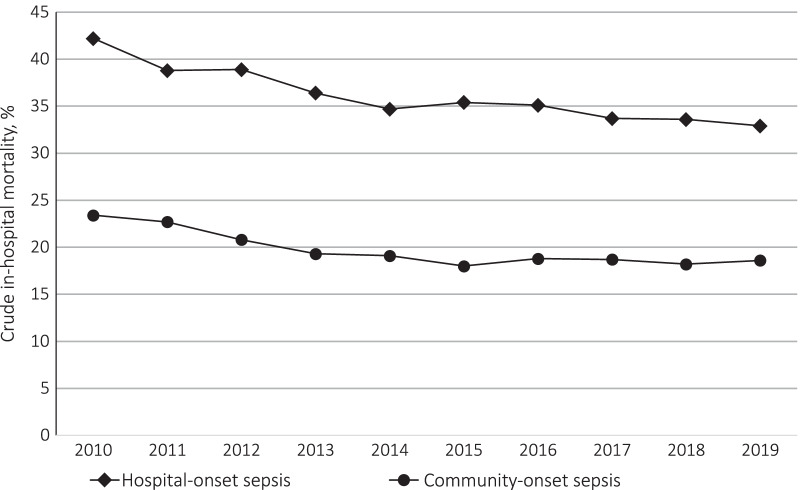
Of 516,124 patients, 52,183 (10.1%) had hospital-onset sepsis and 463,940 (89.9%) had community-onset sepsis. Hospital-onset sepsis was characterized by younger age, infrequent emergency hospitalization, frequent surgery under general anesthesia, and frequent organ support upon critical care unit admission compared to community-onset sepsis. In-hospital mortality was higher for hospital-onset than for community-onset sepsis (35.5% versus 19.2%; unadjusted mean difference, 16.3% [95% confidence interval (CI) 15.9-16.7]; adjusted mean difference, 15.6% [95% CI 14.9-16.2]). Mean hospital length of stay was longer for hospital-onset than for community-onset sepsis (47 days versus 30 days; unadjusted mean difference, 17 days [95% CI 16-17]; adjusted mean difference, 13 days [95% CI 12-14]).
Patients with hospital-onset sepsis admitted to critical care units in Japan had a poorer prognosis and more resource utilization including organ support rate, number of days with critical care unit surcharge codes, and hospital length of stay than those with community-onset sepsis.
医院获得性和社区获得性败血症是重要的败血症亚组。日本比较这些亚组的数据有限。本研究旨在描述日本重症监护病房中医院获得性和社区获得性败血症的流行病学。
我们使用日本诊断和程序组合数据库进行了回顾性队列研究。纳入 2010 年 4 月至 2020 年 3 月因败血症入住重症监护病房的成年患者。败血症病例的确定依据是传染病的 ICD-10 编码、血培养试验的程序代码和抗菌药物的用药代码。评估了患者的特征、住院死亡率和资源利用情况。使用泊松回归广义线性混合效应模型比较两组之间的住院死亡率。
在 516124 名患者中,52183 名(10.1%)患有医院获得性败血症,463940 名(89.9%)患有社区获得性败血症。与社区获得性败血症相比,医院获得性败血症的特点是年龄较小、急诊住院频率较低、全麻下手术频率较高以及入住重症监护病房时器官支持频率较高。医院获得性败血症的住院死亡率高于社区获得性败血症(35.5%比 19.2%;未调整的平均差异为 16.3%[95%置信区间(CI)15.9-16.7];调整后的平均差异为 15.6%[95%CI 14.9-16.2])。医院获得性败血症的平均住院时间长于社区获得性败血症(47 天比 30 天;未调整的平均差异为 17 天[95%CI 16-17];调整后的平均差异为 13 天[95%CI 12-14])。
与社区获得性败血症相比,日本重症监护病房中因医院获得性败血症入院的患者预后较差,资源利用率较高,包括器官支持率、重症监护病房附加费用代码天数和住院时间。