Desantis Vanessa, Savino Francesco Domenico, Scaringella Antonietta, Potenza Maria Assunta, Nacci Carmela, Frassanito Maria Antonia, Vacca Angelo, Montagnani Monica
Department of Biomedical Sciences and Human Oncology, Pharmacology Section, University of Bari Aldo Moro Medical School, 70124 Bari, Italy.
Unit of General Pathology, Department of Biomedical Sciences and Human Oncology, University of Bari Aldo Moro Medical School, 70124 Bari, Italy.
J Clin Med. 2022 Apr 29;11(9):2513. doi: 10.3390/jcm11092513.
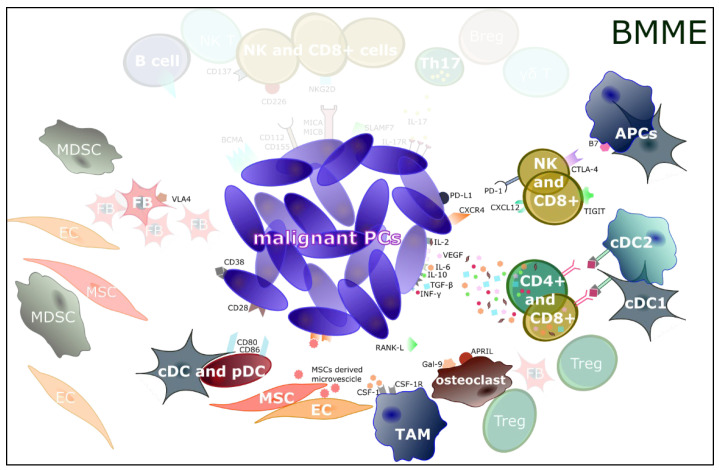
Multiple myeloma (MM) is a plasma cell (PC) malignancy whose development flourishes in the bone marrow microenvironment (BMME). The BMME components' immunoediting may foster MM progression by favoring initial immunotolerance and subsequent tumor cell escape from immune surveillance. In this dynamic process, immune effector cells are silenced and become progressively anergic, thus contributing to explaining the mechanisms of drug resistance in unresponsive and relapsed MM patients. Besides traditional treatments, several new strategies seek to re-establish the immunological balance in the BMME, especially in already-treated MM patients, by targeting key components of the immunoediting process. Immune checkpoints, such as CXCR4, T cell immunoreceptor with immunoglobulin and ITIM domains (TIGIT), PD-1, and CTLA-4, have been identified as common immunotolerance steps for immunotherapy. B-cell maturation antigen (BCMA), expressed on MMPCs, is a target for CAR-T cell therapy, antibody-(Ab) drug conjugates (ADCs), and bispecific mAbs. Approved anti-CD38 (daratumumab, isatuximab), anti-VLA4 (natalizumab), and anti-SLAMF7 (elotuzumab) mAbs interfere with immunoediting pathways. New experimental drugs currently being evaluated (CD137 blockers, MSC-derived microvesicle blockers, CSF-1/CSF-1R system blockers, and Th17/IL-17/IL-17R blockers) or already approved (denosumab and bisphosphonates) may help slow down immune escape and disease progression. Thus, the identification of deregulated mechanisms may identify novel immunotherapeutic approaches to improve MM patients' outcomes.
多发性骨髓瘤(MM)是一种浆细胞(PC)恶性肿瘤,其发展在骨髓微环境(BMME)中蓬勃发展。BMME 成分的免疫编辑可能通过促进初始免疫耐受和随后肿瘤细胞逃避免疫监视来促进 MM 进展。在这个动态过程中,免疫效应细胞被沉默并逐渐变得无反应,从而有助于解释无反应和复发 MM 患者的耐药机制。除了传统治疗方法外,一些新策略试图通过靶向免疫编辑过程的关键成分来重新建立 BMME 中的免疫平衡,特别是在已经接受治疗的 MM 患者中。免疫检查点,如 CXCR4、具有免疫球蛋白和 ITIM 结构域的 T 细胞免疫受体(TIGIT)、PD-1 和 CTLA-4,已被确定为免疫治疗的常见免疫耐受步骤。在多发性骨髓瘤细胞(MMPCs)上表达的 B 细胞成熟抗原(BCMA)是嵌合抗原受体 T 细胞(CAR-T)疗法、抗体-药物偶联物(ADC)和双特异性单克隆抗体的靶点。已获批的抗 CD38(达雷妥尤单抗、isatuximab)、抗 VLA4(那他珠单抗)和抗 SLAMF7(elotuzumab)单克隆抗体可干扰免疫编辑途径。目前正在评估的新实验药物(CD137 阻滞剂、间充质干细胞衍生的微泡阻滞剂、集落刺激因子-1/集落刺激因子-1 受体系统阻滞剂和辅助性 T 细胞 17/白细胞介素-17/白细胞介素-17 受体阻滞剂)或已获批的药物(地诺单抗和双膦酸盐)可能有助于减缓免疫逃逸和疾病进展。因此,识别失调的机制可能有助于确定新的免疫治疗方法,以改善 MM 患者的预后。