Viderman Dmitriy, Tapinova Karina, Nabidollayeva Fatima, Tankacheev Ramil, Abdildin Yerkin G
Department of Biomedical Sciences, Nazarbayev University School of Medicine (NUSOM), Kerei, Zhanibek khandar Str. 5/1, Nur-Sultan 020000, Kazakhstan.
Department of Anesthesiology and Intensive Care, National Research Oncology Center, Kerei, Zhanibek khandar Str. 3, Nur-Sultan 020000, Kazakhstan.
J Clin Med. 2022 May 5;11(9):2579. doi: 10.3390/jcm11092579.
To compare the intravenous and epidural routes of patient-controlled anesthesia in abdominal surgery.
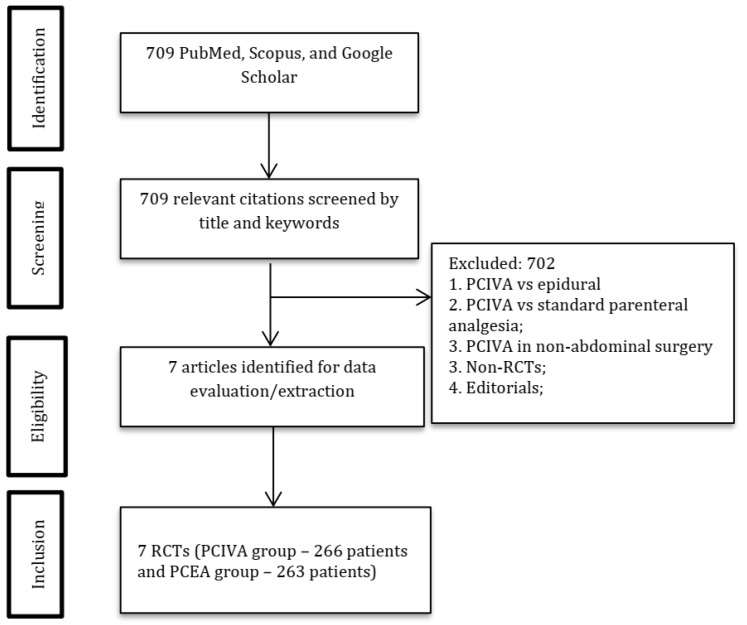
We searched for randomized clinical trials that compared the intravenous and epidural modes of patient-controlled anesthesia in intra-abdominal surgery in adults. Data analysis was performed in RevMan 5.4. Heterogeneity was measured using I statistic. Risk of bias was assessed using the Jadad/Oxford quality scoring system.
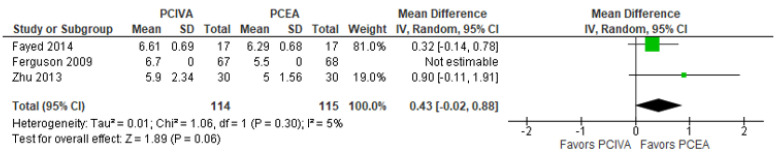
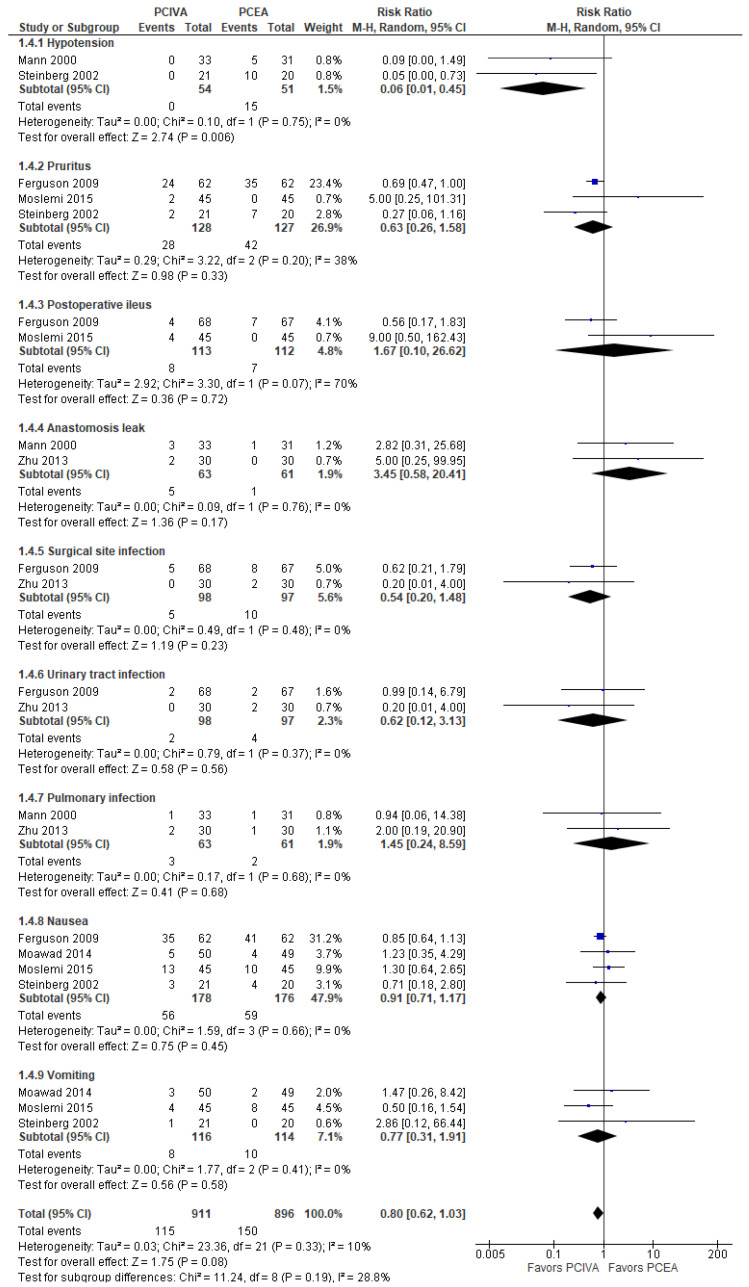
Seven studies reporting 529 patients were included into the meta-analysis. For pain at rest, the mean difference with 95% confidence interval (CI) was -0.00 [-0.79, 0.78], -value 0.99, while for pain on coughing, it was 0.43 [-0.02, 0.88], -value 0.06, indicating that patient-controlled epidural analgesia (PCEA) was superior. For the sedation score, the mean difference with 95% CI was 0.26 [-0.37, 0.89], -value 0.42, slightly favoring PCEA. For the length of hospital stay, the mean difference with 95% CI was 1.13 [0.29, 1.98], -value 0.009, favoring PCEA. For postoperative complications, the risk ratio with 95% CI was 0.8 [0.62, 1.03], -value 0.08, slightly favoring patient-controlled intravenous analgesia (PCIVA). A significant effect was observed for hypotension, favoring PCIVA.
Patient-controlled intravenous analgesia compared with patient-controlled epidural analgesia was associated with fewer episodes of hypotension. PCEA, on other hand, was associated with a shorter length of hospital stay. Pain control and other side effects did not differ significantly. Only three studies out of seven had an acceptable methodological quality. Thus, these conclusions should be taken with caution.
比较腹部手术中静脉自控镇痛和硬膜外自控镇痛两种途径。
我们检索了比较成人腹部手术中静脉自控镇痛和硬膜外自控镇痛模式的随机临床试验。使用RevMan 5.4进行数据分析。采用I统计量测量异质性。使用Jadad/牛津质量评分系统评估偏倚风险。
七项研究共纳入529例患者进行荟萃分析。静息时疼痛的平均差值及95%置信区间(CI)为-0.00 [-0.79, 0.78],P值0.99;咳嗽时疼痛的平均差值及95%CI为0.43 [-0.02, 0.88],P值0.06,表明硬膜外自控镇痛(PCEA)更具优势。镇静评分的平均差值及95%CI为0.26 [-0.37, 0.89],P值0.42,稍有利于PCEA。住院时间的平均差值及95%CI为1.13 [0.29, 1.98],P值0.009,有利于PCEA。术后并发症的风险比及95%CI为0.8 [0.62, 1.03],P值0.08,稍有利于静脉自控镇痛(PCIVA)。低血压方面观察到显著效果,有利于PCIVA。
与硬膜外自控镇痛相比,静脉自控镇痛导致的低血压发作较少。另一方面,PCEA与较短的住院时间相关。疼痛控制和其他副作用无显著差异。七项研究中只有三项具有可接受的方法学质量。因此,这些结论应谨慎对待。