Lincango Naranjo Eddy P, Garces-Delgado Estefany, Siepmann Timo, Mirow Lutz, Solis-Pazmino Paola, Alexander-Leon Harold, Restrepo-Rodas Gabriela, Mancero-Montalvo Rafael, Ponce Cristina J, Cadena-Semanate Ramiro, Vargas-Cordova Ronnal, Herrera-Cevallos Glenda, Vallejo Sebastian, Liu-Sanchez Carolina, Prokop Larry J, Ziogas Ioannis A, Vailas Michail G, Guerron Alfredo D, Visser Brendan C, Ponce Oscar J, Barbas Andrew S, Moris Dimitrios
Knowledge and Evaluation Research Unit, Mayo Clinic, Rochester, MN 55905, USA.
Department of Teaching and Research, Hospital Vozandes Quito, Quito 170521, Ecuador.
J Clin Med. 2022 May 5;11(9):2603. doi: 10.3390/jcm11092603.
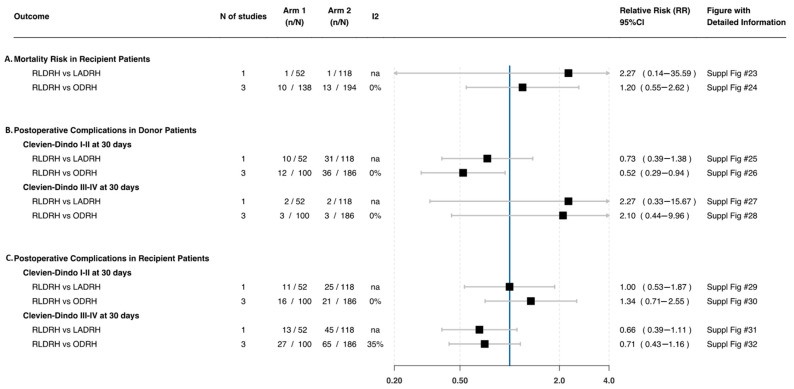
The introduction of robotics in living donor liver transplantation has been revolutionary. We aimed to examine the safety of robotic living donor right hepatectomy (RLDRH) compared to open (ODRH) and laparoscopic (LADRH) approaches. A systematic review was carried out in Medline and six additional databases following PRISMA guidelines. Data on morbidity, postoperative liver function, and pain in donors and recipients were extracted from studies comparing RLDRH, ODRH, and LADRH published up to September 2020; PROSPERO (CRD42020214313). Dichotomous variables were pooled as risk ratios and continuous variables as weighted mean differences. Four studies with a total of 517 patients were included. In living donors, the postoperative total bilirubin level (MD: −0.7 95%CI −1.0, −0.4), length of hospital stay (MD: −0.8 95%CI −1.4, −0.3), Clavien−Dindo complications I−II (RR: 0.5 95%CI 0.2, 0.9), and pain score at day > 3 (MD: −0.6 95%CI −1.6, 0.4) were lower following RLDRH compared to ODRH. Furthermore, the pain score at day > 3 (MD: −0.4 95%CI −0.8, −0.09) was lower after RLDRH when compared to LADRH. In recipients, the postoperative AST level was lower (MD: −0.5 95%CI −0.9, −0.1) following RLDRH compared to ODRH. Moreover, the length of stay (MD: −6.4 95%CI −11.3, −1.5) was lower after RLDRH when compared to LADRH. In summary, we identified low- to unclear-quality evidence that RLDRH seems to be safe and feasible for adult living donor liver transplantation compared to the conventional approaches. No postoperative deaths were reported.
机器人技术在活体肝移植中的应用具有革命性意义。我们旨在研究机器人辅助活体右半肝切除术(RLDRH)与开放手术(ODRH)及腹腔镜手术(LADRH)相比的安全性。按照PRISMA指南,我们在Medline及另外六个数据库中进行了系统综述。从截至2020年9月发表的比较RLDRH、ODRH和LADRH的研究中提取了供体和受体的发病率、术后肝功能及疼痛的数据;国际前瞻性系统评价注册库(PROSPERO,注册号:CRD42020214313)。二分变量合并为风险比,连续变量合并为加权平均差。纳入了四项研究,共517例患者。在活体供体中,与ODRH相比,RLDRH术后总胆红素水平(MD:−0.7,95%CI −1.0,−0.4)、住院时间(MD:−0.8,95%CI −1.4,−0.3)、Clavien-Dindo I-II级并发症(RR:0.5,95%CI 0.2,0.9)及术后3天以上疼痛评分(MD:−0.6,95%CI −1.6,0.4)更低。此外,与LADRH相比,RLDRH术后3天以上疼痛评分(MD:−0.4,95%CI −0.8,−0.09)更低。在受体中,与ODRH相比,RLDRH术后谷草转氨酶水平更低(MD:−0.5,95%CI −0.9,−0.1)。此外,与LADRH相比,RLDRH术后住院时间(MD:−6.4,95%CI −11.3,−1.5)更短。总之,我们发现低质量至质量不明确的证据表明,与传统手术方法相比,RLDRH在成人活体肝移植中似乎是安全可行的。未报告术后死亡病例。