Division of Vascular and Endovascular Surgery, Department of Surgery, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA.
Division of Vascular and Endovascular Surgery, Department of Surgery, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA; Department of Vascular Surgery, University Medical Center, Utrecht, Netherlands.
J Vasc Surg. 2022 Nov;76(5):1205-1215.e4. doi: 10.1016/j.jvs.2022.03.886. Epub 2022 May 13.
Sex, racial, and ethnic disparities in postoperative outcomes following abdominal aortic aneurysm repair have been described, but differences in long-term outcomes are poorly understood. Our aim was to identify differences in 5-year outcomes and imaging surveillance after elective endovascular aortic aneurysm repair (EVAR) by sex, race, and ethnicity and to explore potential mechanisms underlying these differences.
We identified patients undergoing elective EVAR in the Vascular Quality Initiative from 2003 to 2017 with linkage to Medicare claims through 2018 for long-term outcomes. Our primary outcome was 5-year aneurysm rupture. Secondary outcomes were 5-year reintervention and mortality and 2-year loss-to-imaging follow-up (defined as no aortic imaging from 6 to 24 months after EVAR). We used Kaplan-Meier and Cox regression analyses to evaluate these outcomes by sex/race/ethnicity and constructed multivariable models to explore potential contributing factors.
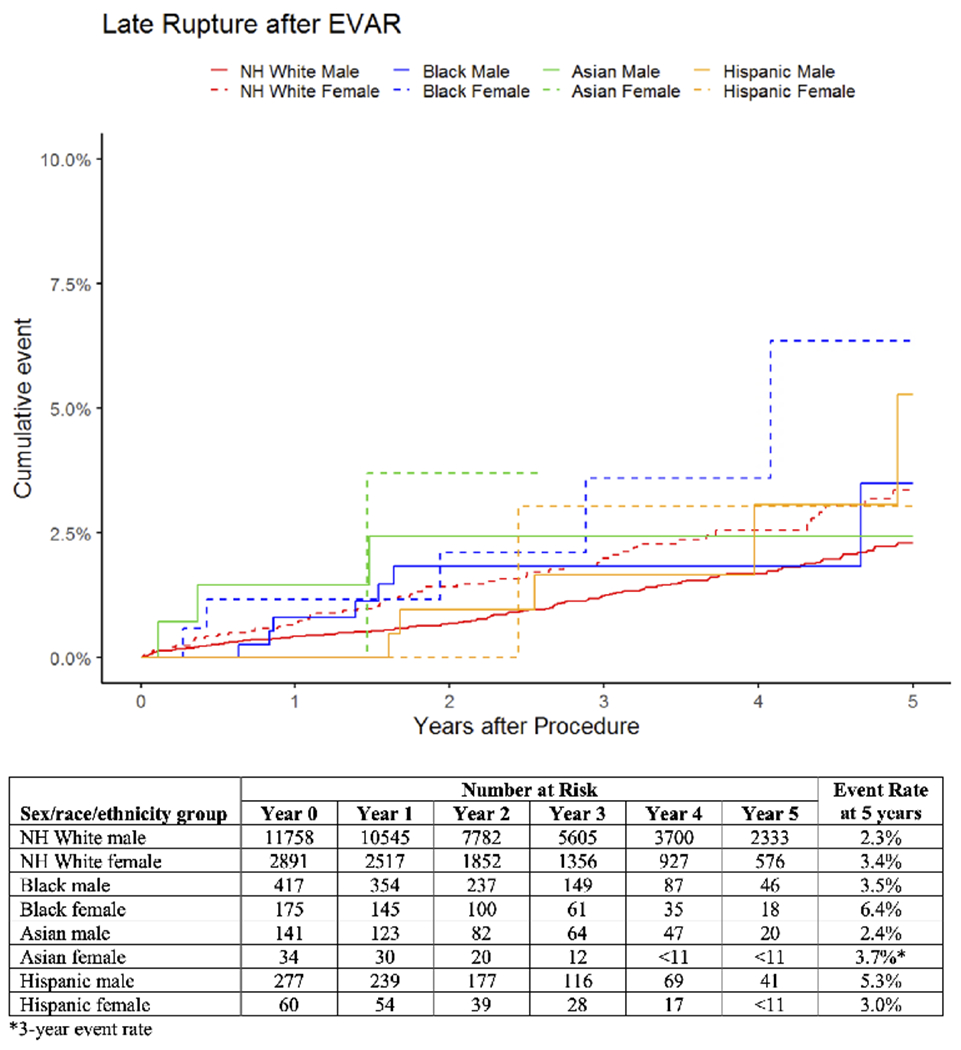
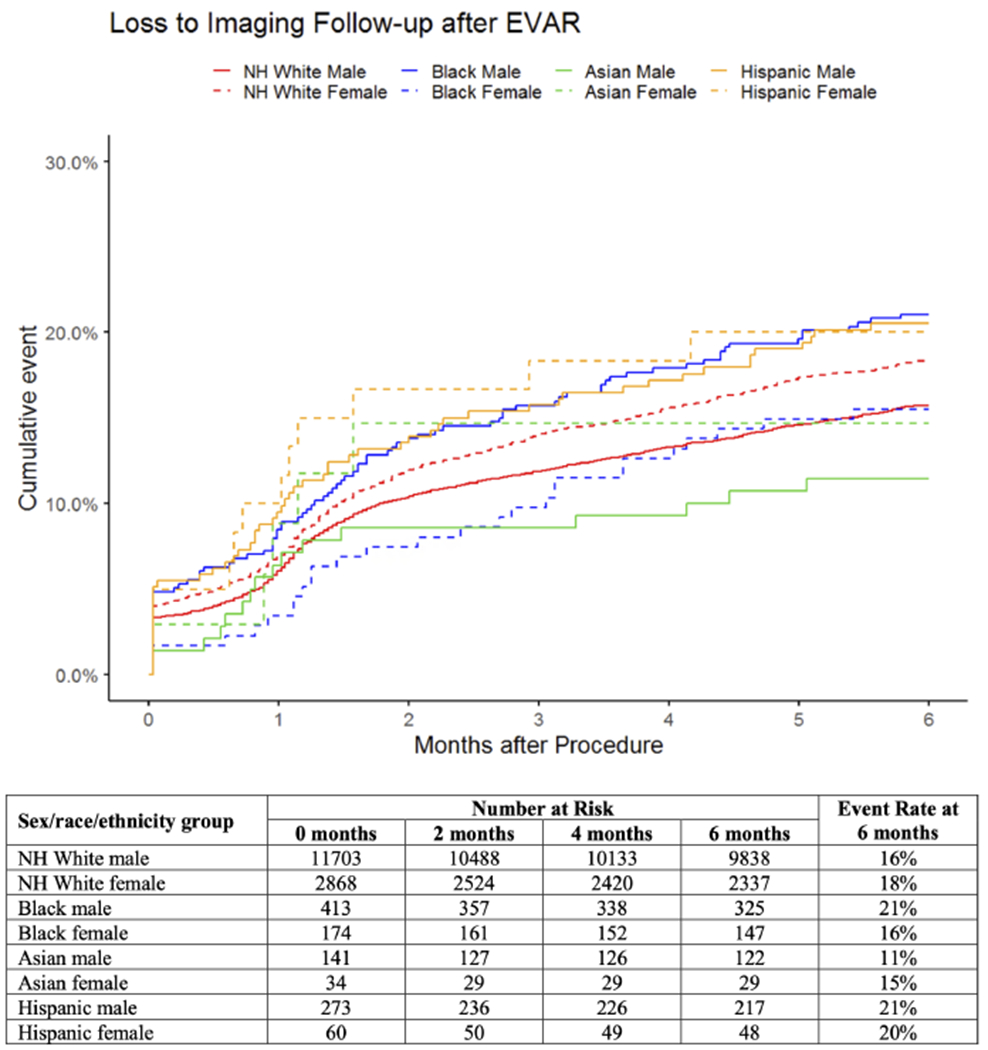
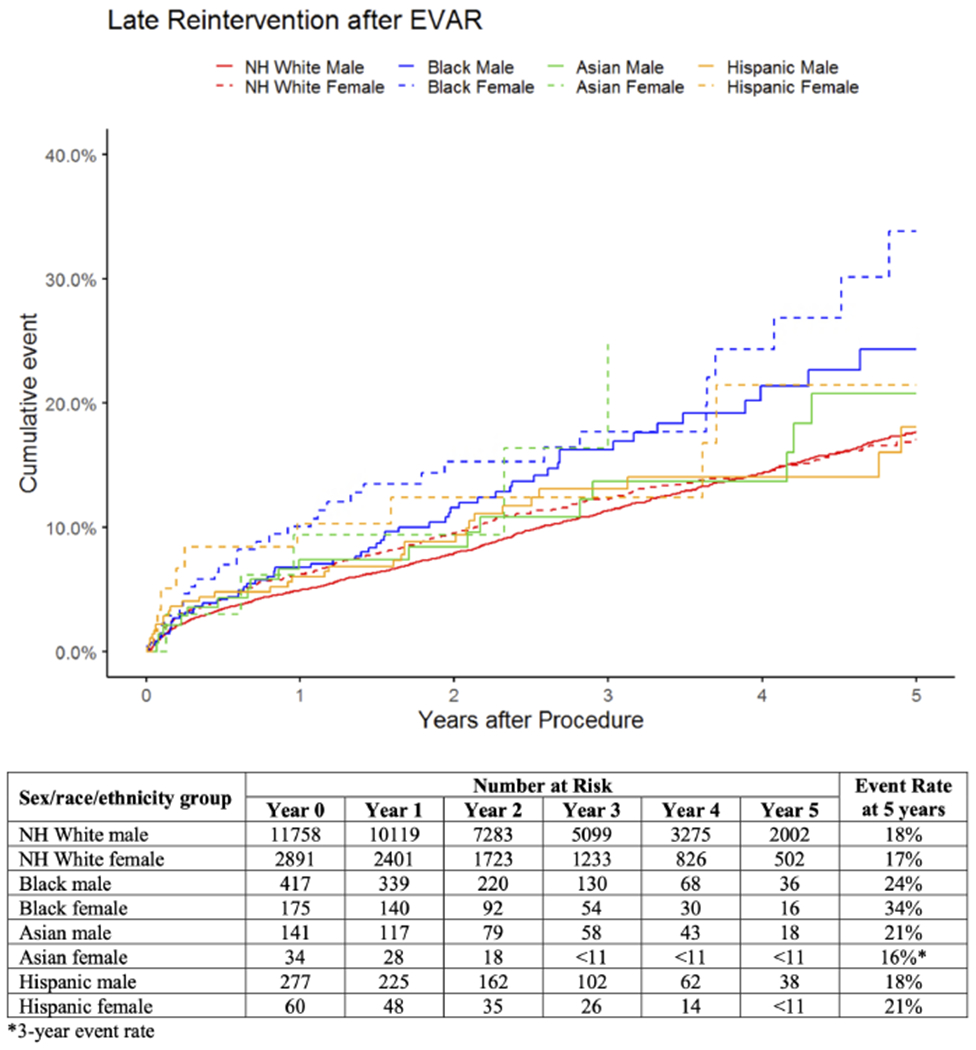
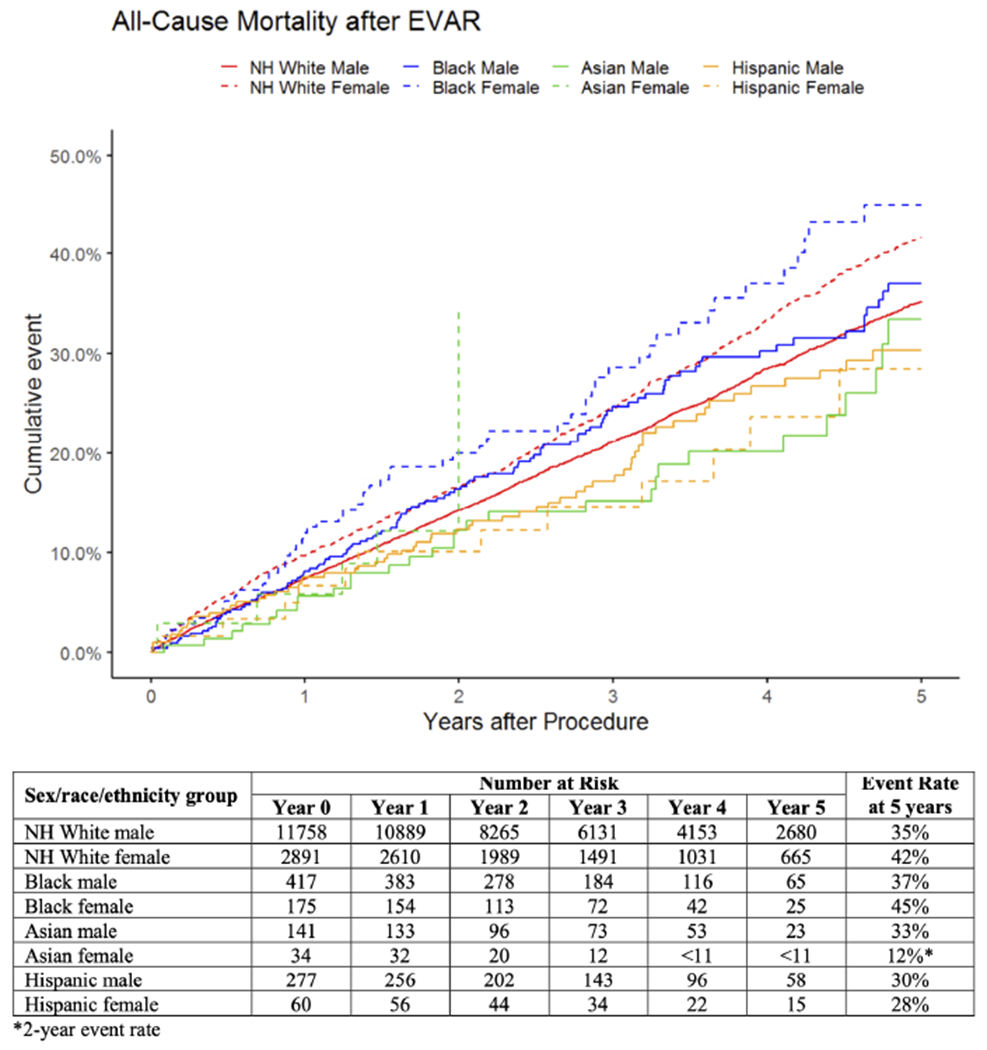
Among 16,040 patients, 11,764 (73%) were White males, 2891 (18%) were White females, 417 (2.6%) were Black males, 175 (1.1%) were Black females, 141 (0.9%) were Asian males, 34 (0.2%) were Asian females, 277 (1.7%) were Hispanic males, and 60 (0.4%) were Hispanic females. At 5 years, rupture rates were highest in Black females at 6.4% and lowest in white males at 2.3%. Compared with White males, rupture rates were higher in White females (hazard ratio [HR], 1.5; 95% confidence interval [CI], 1.1-2.0), Black females (HR, 2.5; 95% CI, 1.0-6.0), and Asian females (HR, 5.2; 95% CI, 1.3-21). White females also had higher mortality (HR, 1.2; 95% CI, 1.2-1.3) and loss-to-imaging-follow-up (HR, 1.2; 95% CI, 1.1-1.3), whereas Black females had higher mortality (HR, 1.4; 95% CI, 1.1-1.8) and reintervention (HR, 2.0; 95% CI, 1.4-2.8). Among other groups, Black males had higher reintervention (HR, 1.4; 95% CI, 1.0-1.8), and both Black and Hispanic males had higher loss-to-imaging-follow-up (Black: HR, 1.4; 95% CI, 1.1-1.7; Hispanic: HR, 1.3; 95% CI, 1.0-1.8). In adjusted analyses, White, Black, and Asian females remained at significantly higher risk for 5-year rupture after accounting for procedure year, clinical and anatomic characteristics, surgeon and hospital volume, and loss-to-imaging follow-up.
Compared with White male patients, Black females had higher 5-year aneurysm rupture, reintervention, and mortality after elective EVAR, whereas White females had higher rupture, mortality and loss-to-imaging-follow-up. Asian females also had higher rupture, and Black males had higher reintervention and loss-to-imaging-follow-up. These populations may benefit from improved preoperative counseling and clinical outreach after EVAR. A larger-scale investigation of current practice patterns and their impact on sex, racial, and ethnic disparities in late outcomes after EVAR is needed to identify tangible targets for improvement.
已描述了腹主动脉瘤修复术后在性别、种族和民族方面的术后结局差异,但对长期结局的差异了解甚少。我们的目的是确定通过性别、种族和民族,在择期血管内修复(EVAR)后 5 年的结果和影像学监测方面存在差异,并探讨潜在的潜在机制。
我们在 2003 年至 2017 年期间从血管质量倡议中确定了接受择期 EVAR 的患者,并通过 2018 年的医疗保险索赔与 Medicare 进行链接,以进行长期结局分析。我们的主要结局是 5 年的动脉瘤破裂。次要结局是 5 年的再次干预和死亡率以及 2 年的影像学随访丢失(定义为 EVAR 后 6 至 24 个月没有主动脉影像学)。我们使用 Kaplan-Meier 和 Cox 回归分析来评估这些结局的性别/种族/民族差异,并构建多变量模型来探索潜在的促成因素。
在 16040 名患者中,11764 名(73%)为白人男性,2891 名(18%)为白人女性,417 名(2.6%)为黑人男性,175 名(1.1%)为黑人女性,141 名(0.9%)为亚裔男性,34 名(0.2%)为亚裔女性,277 名(1.7%)为西班牙裔男性,60 名(0.4%)为西班牙裔女性。在 5 年时,黑人女性的破裂率最高,为 6.4%,白人男性的破裂率最低,为 2.3%。与白人男性相比,白人女性的破裂率更高(危险比[HR],1.5;95%置信区间[CI],1.1-2.0),黑人女性(HR,2.5;95%CI,1.0-6.0)和亚裔女性(HR,5.2;95%CI,1.3-21)。白人女性的死亡率(HR,1.2;95%CI,1.2-1.3)和影像学随访丢失(HR,1.2;95%CI,1.1-1.3)也更高,而黑人女性的死亡率(HR,1.4;95%CI,1.1-1.8)和再次干预(HR,2.0;95%CI,1.4-2.8)更高。在其他群体中,黑人男性的再次干预(HR,1.4;95%CI,1.0-1.8)更高,而黑人男性和西班牙裔男性的影像学随访丢失(黑人:HR,1.4;95%CI,1.1-1.7;西班牙裔:HR,1.3;95%CI,1.0-1.8)更高。在调整分析中,在考虑手术年份、临床和解剖特征、外科医生和医院数量以及影像学随访丢失后,白人、黑人和亚裔女性在 5 年内的动脉瘤破裂风险仍显著更高。
与白人男性患者相比,黑人女性在接受择期 EVAR 后 5 年内的动脉瘤破裂、再次干预和死亡率更高,而白人女性的破裂、死亡率和影像学随访丢失更高。亚裔女性的破裂率也更高,而黑人男性的再次干预和影像学随访丢失更高。这些人群可能需要在 EVAR 后进行更好的术前咨询和临床随访。需要对当前实践模式及其对 EVAR 后晚期结局的性别、种族和民族差异的影响进行更大规模的调查,以确定可改善的具体目标。