The Second Department of Intensive Care Unit, The Second Affiliated Hospital of Anhui Medical University, Hefei, China.
The Laboratory of Cardiopulmonary Resuscitation and Critical Care Medicine, The Second Affiliated Hospital of Anhui Medical University, Hefei, China.
Front Public Health. 2022 Apr 29;10:857368. doi: 10.3389/fpubh.2022.857368. eCollection 2022.
There was considerable debate regarding the effect of mean blood glucose (MBG) and glycemic variability (GV) on the mortality of septic patients. This retrospective cohort study aimed to assess the association between MBG and GV with ICU mortality of sepsis patients and to explore the optimal MBG range.
Sepsis patients were enrolled from the Medical Information Mart for Intensive Care IV database (MIMIC-IV). MBG and glycemic coefficient of variation (Glu) were, respectively, calculated to represent the overall glycemic status and GV during ICU stay. The associations between MBG, Glu, and ICU mortality of the septic patients were assessed by using multivariate logistic regression in different subgroups and the severity of sepsis. Restricted cubic splines evaluated the optimal MBG target.
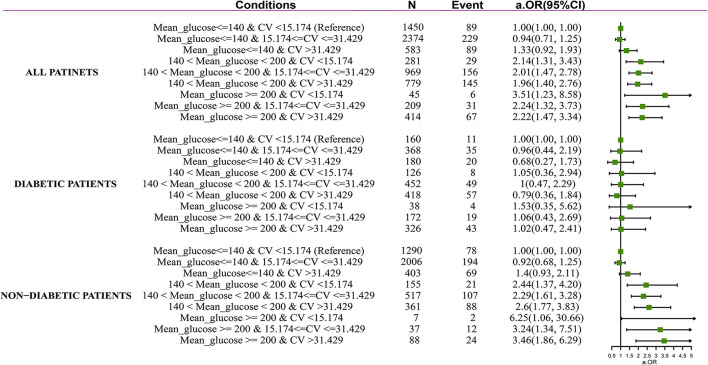
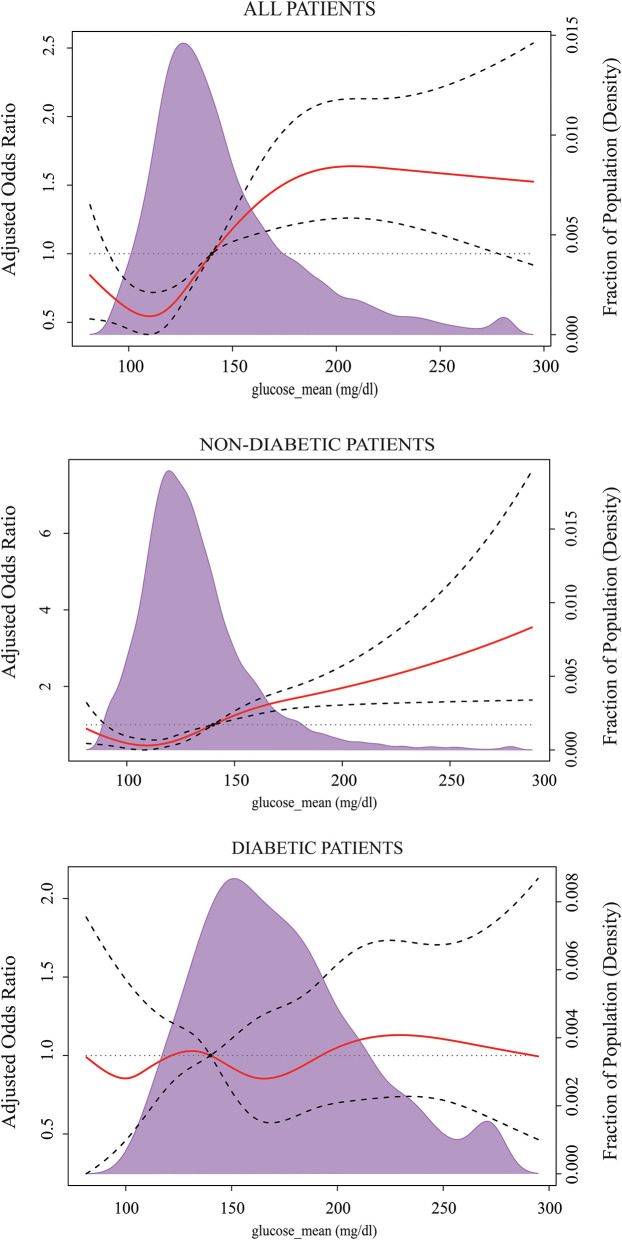
A total of 7,104 adult sepsis patients were included. The multivariate logistic regression results showed that increased MBG and Glu were significantly correlated with ICU mortality. The adjusted odds ratios were 1.14 (95% CI 1.09-1.20) and 1.05 (95% CI 1.00-1.12). However, there was no association between hyperglycemia and ICU mortality among diabetes, liver disease, immunosuppression, and hypoglycemia patients. And the impact of high Glu on ICU mortality was not observed in those with diabetes, immunosuppression, liver disease, and non-septic shock. The ICU mortality risk of severe hyperglycemia (≧200 mg/dl) and high Glu (>31.429%), respectively, elevated 2.30, 3.15, 3.06, and 2.37, 2.79, 3.14-folds in mild (SOFA ≦ 3), middle (SOFA 3-7), and severe group (SOFA ≧ 7). The MBG level was associated with the lowest risk of ICU mortality and hypoglycemia between 120 and 140 mg/dl in the subgroup without diabetes. For the diabetic subset, the incidence of hypoglycemia was significantly reduced when the MBG was 140-190 mg/dl, but a glycemic control target effectively reducing ICU mortality was not observed.
MBG and Glu during the ICU stay were associated with all-cause ICU mortality in sepsis patients; however, their harms are not apparent in some particular subgroups. The impact of hyperglycemia and high GV on death increased with the severity of sepsis. The risk of ICU mortality and hypoglycemia in those with no pre-existing diabetes was lower when maintaining the MBG in the range of 120-140 mg/dl.
关于平均血糖(MBG)和血糖变异性(GV)对脓毒症患者死亡率的影响存在相当大的争议。本回顾性队列研究旨在评估 MBG 和 GV 与脓毒症患者 ICU 死亡率之间的关系,并探讨最佳 MBG 范围。
从 Medical Information Mart for Intensive Care IV 数据库(MIMIC-IV)中招募脓毒症患者。分别计算 MBG 和血糖变异系数(Glu),以分别代表 ICU 期间的整体血糖状态和 GV。使用多变量逻辑回归在不同亚组和脓毒症严重程度下评估 MBG、Glu 与脓毒症患者 ICU 死亡率之间的关系。受限立方样条评估最佳 MBG 目标。
共纳入 7104 例成年脓毒症患者。多变量逻辑回归结果表明,MBG 和 Glu 升高与 ICU 死亡率显著相关。调整后的优势比分别为 1.14(95%CI 1.09-1.20)和 1.05(95%CI 1.00-1.12)。然而,在糖尿病、肝病、免疫抑制和低血糖患者中,高血糖与 ICU 死亡率之间没有关联。在糖尿病、免疫抑制、肝病和非感染性休克患者中,高 Glu 对 ICU 死亡率的影响并不明显。严重高血糖(≧200mg/dl)和高 Glu(>31.429%)的 ICU 死亡率风险分别升高 2.30、3.15、3.06 和 2.37、2.79、3.14 倍,分别在轻度(SOFA ≦ 3)、中度(SOFA 3-7)和重度组(SOFA ≧ 7)。在无糖尿病亚组中,MBG 水平在 120-140mg/dl 之间与 ICU 死亡率最低风险和低血糖相关。对于糖尿病亚组,当 MBG 在 140-190mg/dl 时,低血糖的发生率显著降低,但没有观察到有效降低 ICU 死亡率的血糖控制目标。
脓毒症患者 ICU 期间的 MBG 和 Glu 与全因 ICU 死亡率相关;然而,在某些特定亚组中,其危害并不明显。高血糖和高 GV 对死亡的影响随着脓毒症的严重程度而增加。在没有既往糖尿病的患者中,将 MBG 维持在 120-140mg/dl 范围内时,ICU 死亡率和低血糖的风险较低。