Division of Family Planning, Department of Obstetrics, Gynecology, and Reproductive Biology, Brigham & Women's Hospital, the Planned Parenthood League of Massachusetts, Harvard Medical School, the Department of Global Health and Social Medicine, Harvard Medical School, and Tufts Medical Center Boston, Massachusetts.
Obstet Gynecol. 2022 May 1;139(5):771-780. doi: 10.1097/AOG.0000000000004756. Epub 2022 Apr 5.
To compare immediate initiation with delayed initiation of medication abortion among patients with an undesired pregnancy of unknown location.
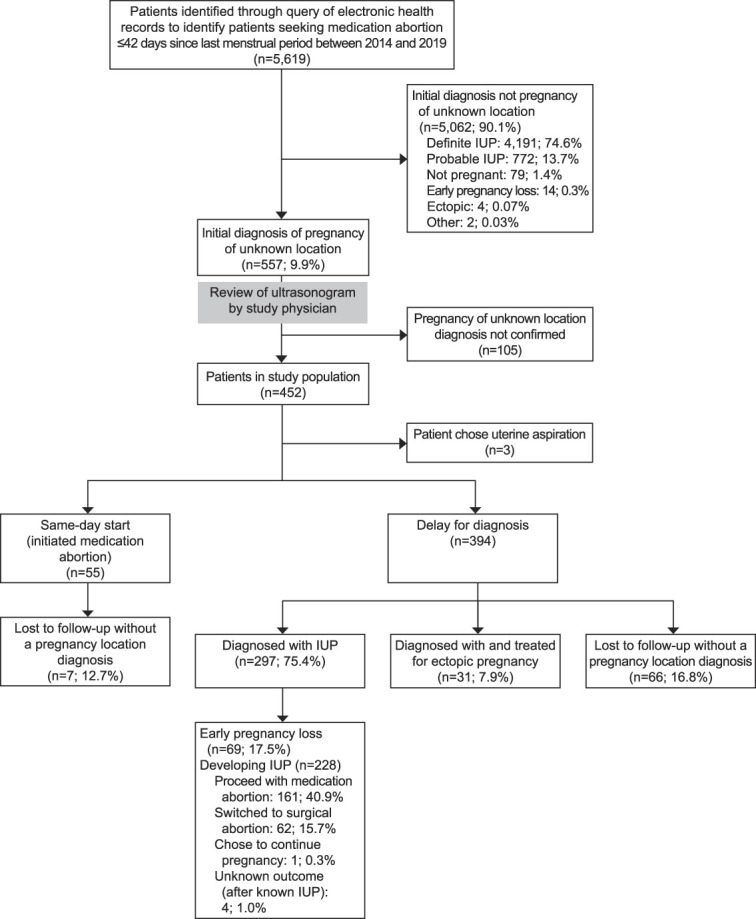
This retrospective cohort study used electronic medical record data from the Planned Parenthood League of Massachusetts (2014-2019) for patients who requested medication abortion with a last menstrual period (LMP) of 42 days or less and pregnancy of unknown location (no gestational sac) on initial ultrasonogram. Clinicians could initiate medication abortion with mifepristone followed by misoprostol while simultaneously excluding ectopic pregnancy with serial serum human chorionic gonadotropin (hCG) testing (same-day-start group) or establish a diagnosis with serial hCG tests and repeat ultrasonogram before initiating treatment (delay-for-diagnosis group). We compared primary safety outcomes (time to diagnosis of pregnancy location [rule out ectopic], emergency department visits, adverse events, and nonadherence with follow-up) between groups. We also reported secondary efficacy outcomes: time to complete abortion, successful medication abortion (no uterine aspiration), and ongoing pregnancy.
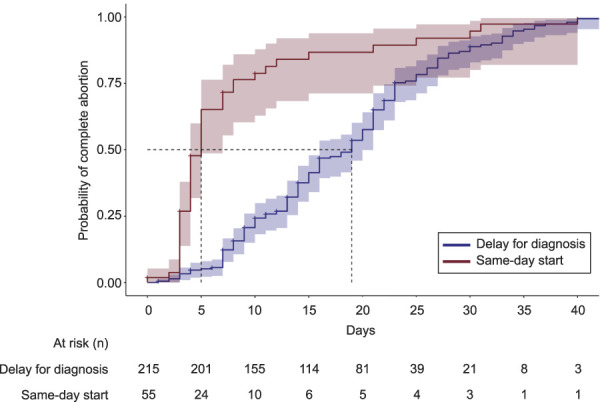
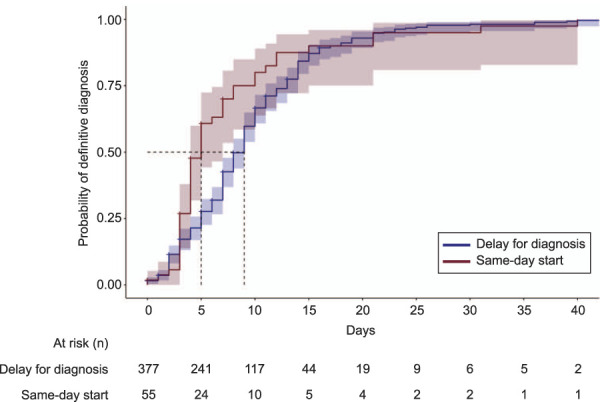
Of 5,619 medication abortion visits for patients with an LMP of 42 days or less, 452 patients had pregnancy of unknown location (8.0%). Three patients underwent immediate uterine aspiration, 55 had same-day start, and 394 had delay for diagnosis. Thirty-one patients (7.9%), all in the delay-for-diagnosis group, were treated for ectopic pregnancy, including four that were ruptured. Among patients with no major ectopic pregnancy risk factors (n=432), same-day start had shorter time to diagnosis (median 5.0 days vs 9.0 days; P=.005), with no significant difference in emergency department visits (adjusted odds ratio [aOR] 0.90, 95% CI 0.43-1.88) or nonadherence with follow-up (aOR 0.92, 95% CI 0.39-2.15). Among patients who proceeded with abortion (n=270), same-day start had shorter time to complete abortion (median 5.0 days vs 19.0 days; P<.001). Of those who had medication abortion with known outcome (n=170), the rate of successful medication abortion was lower (85.4% vs 96.7%; P=.013) and the rate of ongoing pregnancy was higher (10.4% vs 2.5%; P=.041) among patients in the same-day-start group.
In patients with undesired pregnancy of unknown location, immediate initiation of medication abortion is associated with more rapid exclusion of ectopic pregnancy and pregnancy termination but lower abortion efficacy.
比较不明位置妊娠患者中立即启动与延迟启动药物流产的效果。
本回顾性队列研究使用了马萨诸塞州计划生育联盟(2014-2019 年)的电子病历数据,纳入了最后一次月经(LMP)<42 天且妊娠位置不明(无妊娠囊)的药物流产患者。临床医生可以用米非司酮和米索前列醇同时启动药物流产,同时通过连续血清人绒毛膜促性腺激素(hCG)检测排除异位妊娠(同日启动组),或者通过连续 hCG 检测和重复超声检查来确定诊断,然后再开始治疗(延迟诊断组)。我们比较了两组之间的主要安全性结局(妊娠位置排除异位妊娠的时间[排除异位妊娠]、急诊就诊、不良事件和随访不依从)。我们还报告了次要疗效结局:完全流产的时间、药物流产成功(无需子宫抽吸术)和持续妊娠。
在 LMP<42 天的 5619 例药物流产就诊中,有 452 例妊娠位置不明(8.0%)。3 例患者立即接受了子宫抽吸术,55 例患者进行了同日启动,394 例患者进行了延迟诊断。31 例(7.9%)患者,均在延迟诊断组,接受了异位妊娠治疗,其中 4 例为破裂。在无主要异位妊娠危险因素的患者(n=432)中,同日启动的诊断时间更短(中位数 5.0 天 vs 9.0 天;P=0.005),急诊就诊率无显著差异(校正比值比[aOR]0.90,95%置信区间[CI]0.43-1.88)或随访不依从率(aOR 0.92,95%CI 0.39-2.15)。在继续进行流产的患者(n=270)中,同日启动的完成流产时间更短(中位数 5.0 天 vs 19.0 天;P<.001)。在已知结局的患者中(n=170),同日启动组的药物流产成功率较低(85.4% vs 96.7%;P=0.013),持续妊娠率较高(10.4% vs 2.5%;P=0.041)。
在不明位置妊娠患者中,立即启动药物流产与更快排除异位妊娠和终止妊娠有关,但流产效果较低。