Division of Renal Medicine, Department of Medicine, Brigham and Women's Hospital and Harvard Medical School, Boston, Massachusetts.
Division of Nephrology, Department of Medicine, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, Massachusetts.
Kidney360. 2022 Jan 19;3(3):455-464. doi: 10.34067/KID.0007862021. eCollection 2022 Mar 31.
Sodium-glucose cotransporter-2 inhibitors (SGLT-2i) reduce kidney disease progression and mortality in patients with chronic kidney disease (CKD), regardless of diabetes status. However, the prescribing patterns of these novel therapeutics in the CKD population in real-world settings remain largely unknown.
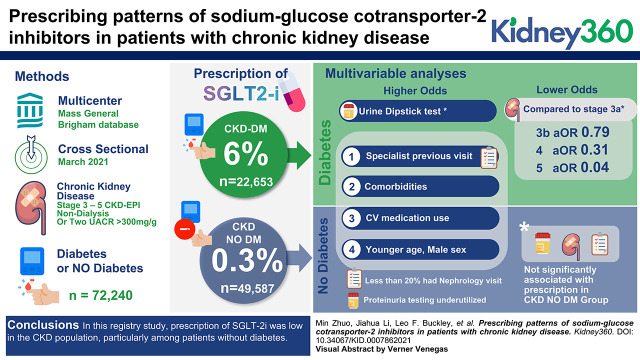
This cross-sectional study included adults with stages 3-5 CKD included in the Mass General Brigham (MGB) CKD registry in March 2021. We described the adoption of SGLT-2i therapy and evaluated factors associated with SGLT-2i prescription using multivariable logistic regression models in the CKD population, with and without diabetes.
A total of 72,240 patients with CKD met the inclusion criteria, 31,688 (44%) of whom were men and 61,265 (85%) White. A total of 22,653 (31%) patients were in the diabetic cohort, and 49,587 (69%) were in the nondiabetic cohort. SGLT-2i prescription was 6% in the diabetic cohort and 0.3% in the nondiabetic cohort. In multivariable analyses, younger Black men with a history of heart failure, use of cardiovascular medications, and at least one cardiologist visit in the previous year were associated with higher odds of SGLT-2i prescription in both diabetic and nondiabetic cohorts. Among patients with diabetes, advanced CKD stages were associated with lower odds of SGLT-2i prescription, whereas urine dipstick test and at least one subspecialist visit in the previous year were associated with higher odds of SGLT-2i prescription. In the nondiabetic cohort, CKD stage, urine dipstick test, and at least one nephrologist visit in the previous year were not significantly associated with SGLT-2i prescription.
In this registry study, prescription of SGLT-2i was low in the CKD population, particularly among patients without diabetes.
钠-葡萄糖共转运蛋白 2 抑制剂(SGLT-2i)可降低慢性肾脏病(CKD)患者的肾脏疾病进展和死亡率,无论其糖尿病状态如何。然而,在真实环境下 CKD 人群中这些新型治疗药物的处方模式在很大程度上仍是未知的。
本横断面研究纳入了 2021 年 3 月纳入麻省总医院布里格姆(MGB)CKD 登记处的 3-5 期 CKD 成年患者。我们描述了 SGLT-2i 治疗的采用情况,并使用多变量逻辑回归模型在 CKD 人群中(无论是否患有糖尿病)评估了与 SGLT-2i 处方相关的因素。
共有 72240 名 CKD 患者符合纳入标准,其中 31688 名(44%)为男性,61265 名(85%)为白人。共有 22653 名(31%)患者为糖尿病队列,49587 名(69%)为非糖尿病队列。糖尿病队列中 SGLT-2i 处方率为 6%,非糖尿病队列中为 0.3%。在多变量分析中,年轻黑人男性,有心力衰竭史,使用心血管药物,以及在过去一年中有至少一次看心脏病专家的就诊,与糖尿病和非糖尿病队列中 SGLT-2i 处方的更高几率相关。在患有糖尿病的患者中,更严重的 CKD 阶段与 SGLT-2i 处方的几率降低相关,而尿试纸检查和在过去一年中有至少一次看肾脏病专家的就诊与 SGLT-2i 处方的几率增加相关。在非糖尿病队列中,CKD 阶段、尿试纸检查和在过去一年中有至少一次看肾脏病专家的就诊与 SGLT-2i 处方无显著相关性。
在这项登记研究中,CKD 人群中 SGLT-2i 的处方率较低,特别是在没有糖尿病的患者中。