The Berman Center for Outcomes and Clinical Research, Hennepin Healthcare Research Institute, Minneapolis, Minnesota.
Department of Medicine, Geriatrics Division, Hennepin Healthcare, Minneapolis, Minnesota.
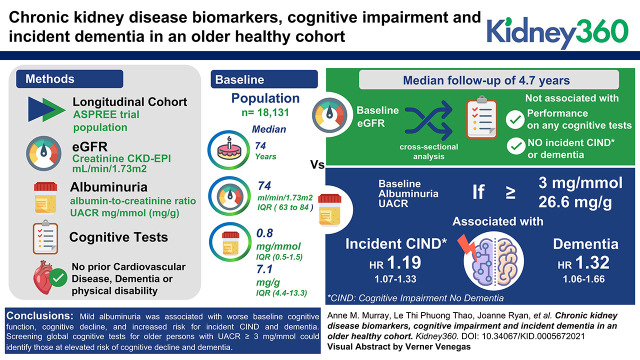
Kidney360. 2021 Dec 7;3(3):435-445. doi: 10.34067/KID.0005672021. eCollection 2022 Mar 31.
CKD is a risk factor for cognitive impairment (CI), but reports of individual associations of eGFR and albuminuria with CI and incident dementia in healthier, older, longitudinal populations are lacking. Our goal was to estimate these associations in a large cohort of older healthy persons.
In a longitudinal cohort study of older persons without prior cardiovascular disease, we estimated the associations between baseline eGFR (in ml/min per 1.73 m) and albuminuria, measured as urine albumin-creatinine ratio (UACR; in mg/mmol) and cognitive test scores, declines in cognitive test scores, and incident dementia using adjusted linear and linear mixed models. Cox proportional hazards regression models assessed the association between baseline kidney function and incident CI no dementia (CIND) or dementia at a median of 4.7 years.
At baseline, among 18,131 participants, median age was 74 years, eGFR was 74 (IQR, 63-84) ml/min per 1.73 m, UACR was 0.8 (IQR, 0.5-1.5) mg/mmol (7.1 [4.4-13.3] mg/g), and 56% were female. Baseline eGFR was not associated with performance on any cognitive tests in cross-sectional analysis, nor was incident CIND or dementia over a median follow-up of 4.7 years. However, baseline UACR ≥3 mg/mmol (≥26.6 mg/g) was significantly associated with lower baseline scores and larger declines on the Modified Mini-Mental State Exam, verbal memory and processing speed tests, and with incident CIND (hazard ratio [HR], 1.19; 95% CI, 1.07 to 1.33) and dementia (HR, 1.32; 95% CI, 1.06 to 1.66).
Mild albuminuria was associated with worse baseline cognitive function, cognitive decline, and increased risk for incident CIND and dementia. Screening global cognitive tests for older persons with UACR 3 mg/mmol could identify those at elevated risk of cognitive decline and dementia.
CKD 是认知障碍(CI)的一个危险因素,但缺乏关于 eGFR 和白蛋白尿与 CI 和在更健康、年龄更大的纵向人群中发生痴呆的个体相关性的报告。我们的目标是在一个大型老年健康人群队列中估计这些相关性。
在一项无先前心血管疾病的老年人群的纵向队列研究中,我们使用调整后的线性和线性混合模型,估计基线时 eGFR(以每 1.73m 毫升/分钟表示)和白蛋白尿(以尿白蛋白/肌酐比值[UACR]表示)与认知测试分数、认知测试分数下降以及 4.7 年中位时间内发生痴呆的相关性。Cox 比例风险回归模型评估了基线肾脏功能与无痴呆的 CI (CIND)或痴呆的发生风险之间的相关性。
在 18131 名参与者中,基线时的中位年龄为 74 岁,eGFR 为 74(IQR,63-84)毫升/分钟/1.73m,UACR 为 0.8(IQR,0.5-1.5)mg/mmol(7.1[4.4-13.3]mg/g),56%为女性。横断面分析显示,基线 eGFR 与任何认知测试的表现均无相关性,在中位随访 4.7 年后也未发生新发 CIND 或痴呆。然而,基线 UACR≥3mg/mmol(≥26.6mg/g)与较低的基线得分和改良的简易精神状态检查、语言记忆和处理速度测试的更大下降有关,与新发 CIND(风险比[HR],1.19;95%置信区间[CI],1.07 至 1.33)和痴呆(HR,1.32;95%CI,1.06 至 1.66)相关。
轻度白蛋白尿与基线认知功能较差、认知下降以及新发 CIND 和痴呆的风险增加相关。对 UACR 为 3mg/mmol 的老年患者进行全球认知测试筛查,可识别出认知能力下降和痴呆风险升高的患者。