Australian Institute of Health Innovation, Macquarie University, Sydney, New South Wales, Australia
Australian Institute of Health Innovation, Macquarie University, Sydney, New South Wales, Australia.
BMJ Open. 2022 May 19;12(5):e058158. doi: 10.1136/bmjopen-2021-058158.
Realist synthesis.
Large-scale hospital improvement initiatives can standardise healthcare across multiple sites but results are contingent on the implementation strategies that complement them. The benefits of these implemented interventions are rarely able to be replicated in different contexts. Realist studies explore this phenomenon in depth by identifying underlying context-mechanism-outcome interactions.
To review implementation strategies used in large-scale hospital initiatives and hypothesise initial programme theories for how they worked across different contexts.
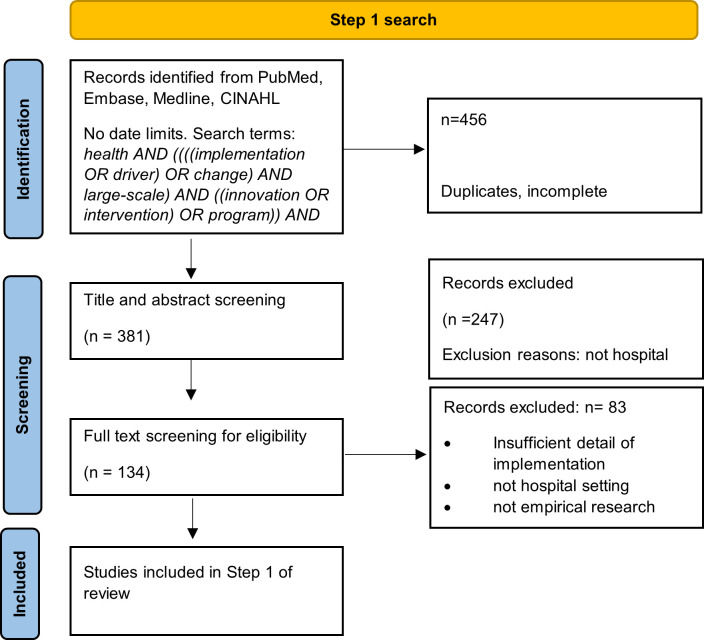
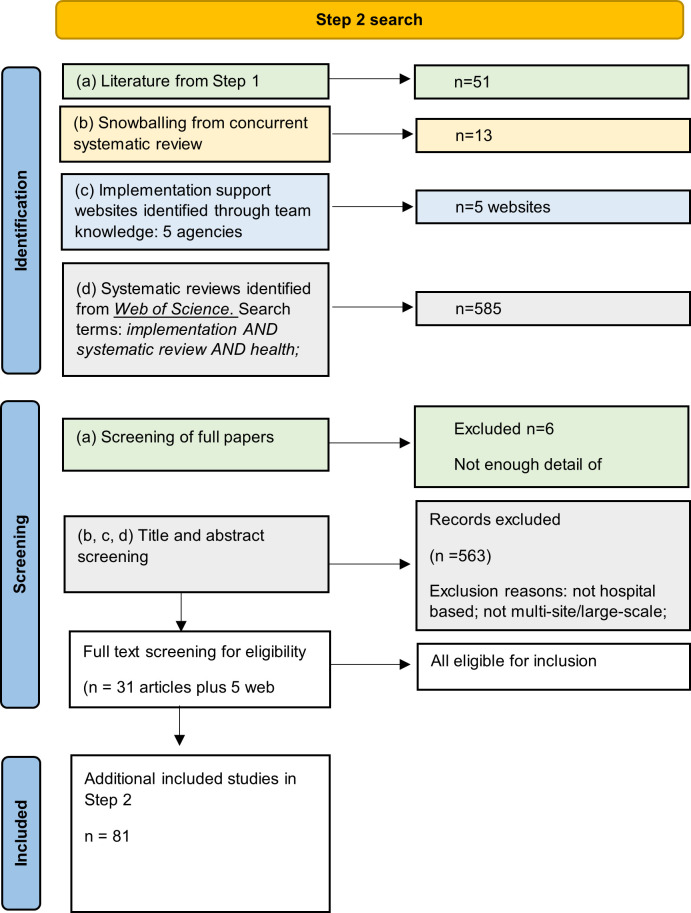
An iterative, four-step process was applied. Step 1 explored the concepts inherent in large-scale interventions using database searches and snowballing. Step 2 identified strategies used in their implementation. Step 3 identified potential initial programme theories that may explain strategies' mechanisms. Step 4 focused on one strategy-theory pairing to develop and test context-mechanism-outcome hypotheses. Data was drawn from searches (March-May 2020) of MEDLINE, Embase, PubMed and CINAHL, snowballed from key papers, implementation support websites and the expertise of the research team and experts.
reported implementation of a large-scale, multisite hospital intervention. RAMESES reporting standards were followed.
Concepts were identified from 51 of 381 articles. Large-scale hospital interventions were characterised by a top-down approach, external and internal support and use of evidence-based interventions. We found 302 reports of 28 different implementation strategies from 31 reviews (from a total of 585). Formal theories proposed for the implementation strategies included Diffusion of Innovation, and Organisational Readiness Theory. Twenty-three context-mechanism-outcome statements for implementation strategies associated with planning and assessment activities were proposed. Evidence from the published literature supported the hypothesised programme theories and were consistent with Organisational Readiness Theory's tenets.
This paper adds to the literature exploring why large-scale hospital interventions are not always successfully implemented and suggests 24 causative mechanisms and contextual factors that may drive outcomes in the planning and assessment stage.
现实主义综合研究。
大型医院改进计划可以在多个地点规范医疗保健,但结果取决于补充这些计划的实施策略。这些实施干预措施的好处很少能够在不同的环境中复制。现实主义研究通过识别潜在的背景-机制-结果相互作用,深入探讨了这一现象。
审查大型医院计划中使用的实施策略,并假设它们在不同背景下运作的初步计划理论。
应用了一个迭代的四步过程。第 1 步使用数据库搜索和滚雪球法探索大型干预措施中固有的概念。第 2 步确定在实施中使用的策略。第 3 步确定可能解释策略机制的初步计划理论。第 4 步专注于一个策略-理论配对,以开发和测试背景-机制-结果假设。数据来自于 2020 年 3 月至 5 月对 MEDLINE、Embase、PubMed 和 CINAHL 的搜索、关键论文的滚雪球、实施支持网站以及研究团队和专家的专业知识。
报告大型多地点医院干预的实施情况。遵循 RAMESES 报告标准。
从 381 篇文章中识别出 51 个概念。大型医院干预的特点是自上而下的方法、外部和内部支持以及使用基于证据的干预措施。我们从 31 篇综述中找到了 28 种不同实施策略的 302 份报告(总计 585 份)。为实施策略提出的正式理论包括创新扩散和组织准备理论。提出了 23 个与规划和评估活动相关的实施策略的背景-机制-结果陈述。来自已发表文献的证据支持假设的计划理论,并且与组织准备理论的原则一致。
本文增加了探索为什么大型医院干预措施并不总是成功实施的文献,并提出了 24 个因果机制和可能在规划和评估阶段驱动结果的背景因素。