Christiansen Ola, Bratt Ola, Kirkevold Øyvind, Benth Jūratė Šaltytė, Manoharan Pathmakulendran, Selnes Anders, Haug Erik Skaaheim, Slaaen Marit
The Research Centre for Age Related Functional Decline and Diseases, Innlandet Hospital Trust, Ottestad, Norway.
Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway.
Cent European J Urol. 2022;75(1):35-40. doi: 10.5173/ceju.2021.0217. Epub 2022 Dec 31.
Prostate-specific antigen (PSA) density has previously been identified as a predictor of histological upgrading at radical prostatectomy, but how information from pre-treatment biparametric magnetic resonance imaging (bpMRI) contributes needs further clarification. The objective of this register-based study was to identify predictors of upgrading at prostatectomy in men with Grade group (GG) 1 and pre-treatment bpMRI.
This single-center study included men with GG 1 cancer on prediagnostic biopsy, who underwent bpMRI and robotic-assisted radical prostatectomy (RARP) between March 2014 and September 2019. We estimated logistic regression models to explore predictors for upgrading. The explored potential predictors were age, PSA density, tumor stage and Prostate Imaging Reporting and Data System (PI-RADS) score (dichotomised 1-3 versus 4-5).
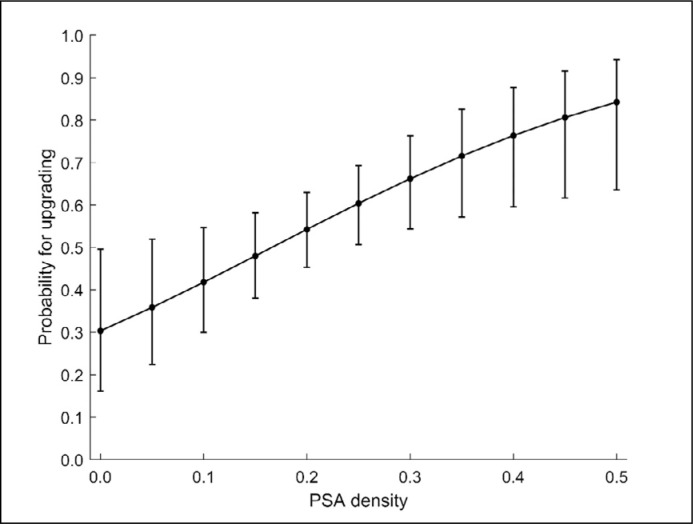
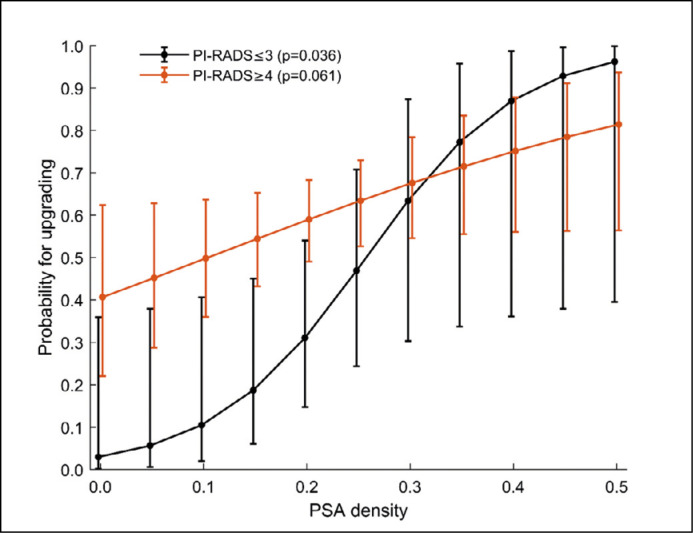
Upgrading was observed in 56% (73/130) of the men. PSA density was the only significant predictor for upgrading (unadjusted OR = 1.7, 95% CI 1.2; 2.4 adjusted OR = 1.7, 95% CI 1.2; 2.5). The probability of upgrading was lower for men with a PIRADS 1-3 than for PIRADS 4-5, but the difference was not statistically significant (adjusted OR 0.4, 95% CI 0.2; 1.1, p = 0.082). Among men with PI-RADS 1-3, the probability increased with increasing PSA density (p = 0.036). With PI-RADS 4-5 the probability of upgrading was high over the entire PSA density range.
PSA density is a clinically important factor to predict upgrading from GG1 when bpMRI shows PI-RADS 1-3. In men with PI-RADS 4-5 on bpMRI, the probability of an undetected GG 2-5 cancer is high regardless of the PSA density.
前列腺特异性抗原(PSA)密度先前已被确定为根治性前列腺切除术中组织学升级的预测指标,但来自治疗前双参数磁共振成像(bpMRI)的信息如何发挥作用仍需进一步阐明。这项基于登记的研究的目的是确定1级组(GG)且有治疗前bpMRI的男性患者前列腺切除术中升级的预测指标。
这项单中心研究纳入了在诊断前活检中患有GG 1期癌症、于2014年3月至2019年9月期间接受bpMRI和机器人辅助根治性前列腺切除术(RARP)的男性患者。我们估计了逻辑回归模型以探索升级的预测指标。所探索的潜在预测指标包括年龄、PSA密度、肿瘤分期和前列腺影像报告和数据系统(PI-RADS)评分(分为1-3与4-5两组)。
56%(73/130)的男性患者出现了升级情况。PSA密度是升级的唯一显著预测指标(未调整的比值比=1.7,95%置信区间1.2;2.4;调整后的比值比=1.7,95%置信区间1.2;2.5)。PI-RADS 1-3的男性患者升级的概率低于PI-RADS 4-5的患者,但差异无统计学意义(调整后的比值比0.4,95%置信区间0.2;1.1,p = 0.082)。在PI-RADS 1-3的男性患者中,升级概率随PSA密度增加而升高(p = 0.036)。对于PI-RADS 4-5的患者,在整个PSA密度范围内升级概率都很高。
当bpMRI显示PI-RADS 1-3时,PSA密度是预测从GG1升级的一个临床重要因素。对于bpMRI显示PI-RADS 4-5的男性患者,无论PSA密度如何,未检测到GG 2-5期癌症的概率都很高。