Centre for Research on Health Care in Disasters, Department of Global Public Health, Karolinska Institutet, Stockholm, Sweden.
World Health Organization Country Office, Beirut, Lebanon.
Prehosp Disaster Med. 2022 Aug;37(4):529-534. doi: 10.1017/S1049023X22000784. Epub 2022 May 20.
On August 4, 2020, a massive explosion struck the Beirut Harbor in Lebanon. Approximately 220 people were killed and around 7,000 were injured, of which 12% were hospitalized. Despite being weakened by economic crisis and increasing numbers of coronavirus disease 2019 (COVID-19) cases, the national health care system responded promptly. Within a day, international health care assistance in the form of International Emergency Medical Teams (I-EMTs) started arriving. Previous studies have found that I-EMTs have arrived late and have not been adapted to the context and dominating health care needs. The aim of this study was to document the organization, type, activity, and timing of I-EMTs deployed to Beirut and to discuss their relevance in relation to medical needs.
Data on all deployed I-EMTs were retrieved from all available sources, including internet searches, I-EMT contacts, and from the World Health Organization (WHO) EMT coordination cell (EMT CC) in Lebanon. The WHO EMT classification was used to categorize deployed teams. Information on characteristics, timing, and activities was retrieved and systematically assessed.
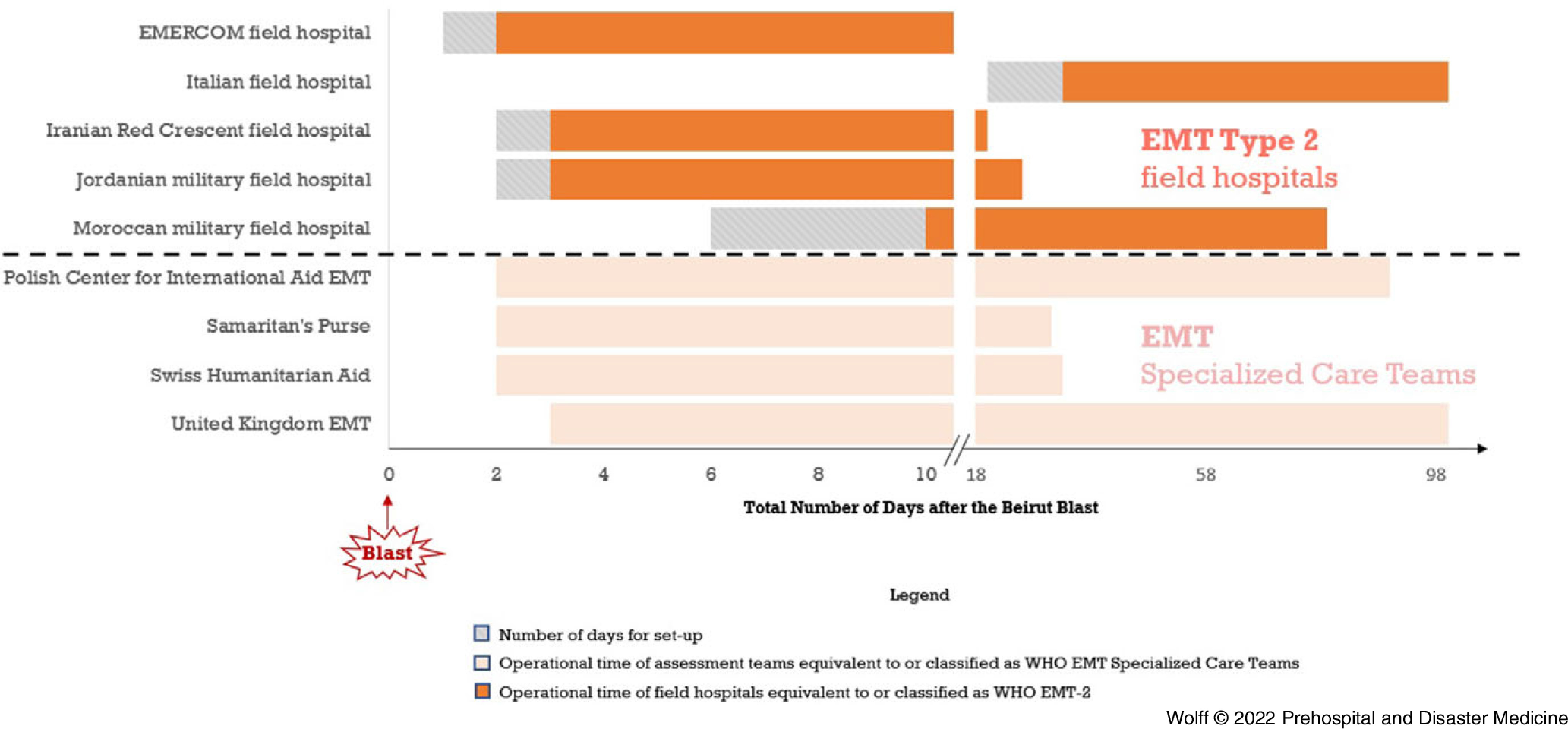
Nine I-EMTs were deployed to Beirut following the explosion. Five were equivalent to EMT Type 2 (field hospitals), out of which three were military. The first EMT Type 2 arrived within 24 hours, while the last EMT set up one month after the explosion. Four civilian I-EMTs provided non-clinical support as EMT Specialized Care Teams. A majority of the I-EMTs were focused on trauma care. Three of the four I-EMT Specialized Care Teams were rapidly re-tasked to support COVID-19 care in public hospitals.
A majority of the deployed I-EMT Type 2 were military and focused on trauma care rather than the normal burden of disease including COVID-19. Re-tasking of EMTs requires flexible EMTs. To be better adapted, the I-EMT response should be guided by a systematic assessment of both health care capacities in the affected country as well as the varying health effects of hazards before deployment.
2020 年 8 月 4 日,黎巴嫩贝鲁特港发生大规模爆炸。约有 220 人死亡,约 7000 人受伤,其中 12%住院。尽管国家卫生保健系统正受到经济危机和不断增加的 2019 年冠状病毒病(COVID-19)病例的影响,但它还是迅速做出了反应。在一天内,以国际紧急医疗队(I-EMTs)形式的国际医疗援助开始抵达。先前的研究发现,I-EMTs 到达较晚,并且没有适应当地情况和主导的医疗保健需求。本研究的目的是记录部署到贝鲁特的 I-EMTs 的组织、类型、活动和时间,并讨论它们与医疗需求的相关性。
从所有可用来源检索所有部署的 I-EMTs 的数据,包括互联网搜索、I-EMT 联系人以及黎巴嫩世界卫生组织(WHO) EMT 协调小组(EMT CC)。使用 WHO EMT 分类对部署的团队进行分类。检索并系统评估有关特征、时间和活动的信息。
爆炸发生后,有 9 支 I-EMTs 被部署到贝鲁特。其中 5 支相当于 EMT 类型 2(野战医院),其中 3 支是军队。第一支 EMT 类型 2 在 24 小时内到达,而最后一支 EMT 在爆炸一个月后才设立。四支民用 I-EMTs 作为 EMT 专门护理团队提供非临床支持。大多数 I-EMTs 专注于创伤护理。四支 I-EMT 专门护理团队中的三支迅速被重新分配任务,以支持公立医院的 COVID-19 护理。
大多数部署的 EMT 类型 2 是军队,专注于创伤护理,而不是包括 COVID-19 在内的正常疾病负担。重新分配 EMT 需要灵活的 EMT。为了更好地适应,I-EMT 应对措施应根据受灾国的医疗保健能力以及部署前危害的不同健康影响进行系统评估。