Department of Surgery, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania.
Department of Surgery, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania.
J Surg Res. 2022 Oct;278:57-63. doi: 10.1016/j.jss.2022.04.042. Epub 2022 May 17.
Surgical risk calculators have expanded in both number and sophistication of their predictive approach. These calculators are gaining popularity as validated tools to help surgeons estimate mortality and complications following emergency general surgery (EGS). However, the accuracy of risk estimates generated by these calculators compared to risk estimation by practicing surgeons has not been explored.
Acute care surgeons at a quaternary care center prospectively estimated 30-d mortality and complications for adult EGS patients (2019-2021). Surgeon predictions were compared to Predictive OpTimal Trees in Emergency Surgery Risk (POTTER) and NSQIP estimates. Observed-to-expected (O:E) ratios of median aggregate estimates were calculated. C-statistics for surgeon and calculator estimations were utilized to quantify predictive accuracy.
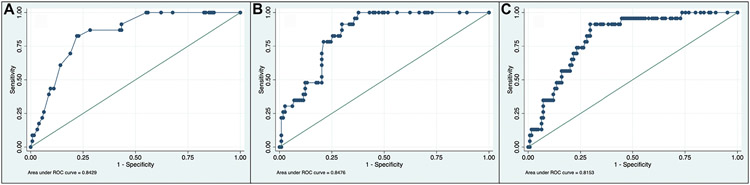
Among 150 patients (median 61 y, 45% male), 30-d mortality was 15% (n = 23). Observed rates of prolonged mechanical ventilation and acute renal failures were 30% and 10%, respectively. Overall, surgeon predictions were similar to risk calculator estimates for mortality (c-statistics 0.843 [surgeon] versus 0.848 [POTTER] and 0.815 [NSQIP]) and need for prolonged ventilation (c-statistics 0.801 versus 0.722 and 0.689, respectively). Surgeons tended to overestimate complication risks. Surgeon experience was not significantly associated with mortality prediction in an adjusted model.
Acute care surgeons at a quaternary care center predicted postoperative mortality and complications with similar discrimination when compared to surgical risk calculators. Surgeon expertise should be utilized in conjunction with risk calculators when counseling EGS patients regarding anticipated postoperative outcomes. Surgeons should be cognizant of patterns in overestimation or underestimation of complications.
外科风险计算器在数量和预测方法的复杂性上都有所增加。这些计算器作为验证工具越来越受欢迎,可以帮助外科医生估计急诊普通外科(EGS)后的死亡率和并发症。然而,这些计算器生成的风险估计与执业外科医生的风险估计相比的准确性尚未得到探索。
一家四级保健中心的急症外科医生前瞻性地估计了成人 EGS 患者的 30 天死亡率和并发症(2019-2021 年)。将外科医生的预测与预测最优树在紧急手术风险(POTTER)和 NSQIP 估计进行比较。计算了中位数综合估计的观察到的预期(O:E)比值。利用外科医生和计算器估计的 C 统计量来量化预测准确性。
在 150 名患者中(中位数 61 岁,45%为男性),30 天死亡率为 15%(n=23)。长时间机械通气和急性肾功能衰竭的观察发生率分别为 30%和 10%。总的来说,外科医生的预测与风险计算器对死亡率(C 统计量 0.843[外科医生]与 0.848[POTTER]和 0.815[NSQIP])和需要长时间通气(C 统计量 0.801 与 0.722 和 0.689,分别)的估计相似。外科医生往往高估并发症风险。在调整后的模型中,外科医生的经验与死亡率预测没有显著相关性。
在一家四级保健中心,急症外科医生在预测术后死亡率和并发症方面的区分能力与外科风险计算器相似。在为 EGS 患者提供预期术后结果的咨询时,应将外科医生的专业知识与风险计算器结合使用。外科医生应该意识到并发症的高估或低估模式。