Azijli Kaoutar, Minderhoud Tanca C, de Gans Carlijn J, Lieveld Arthur W E, Nanayakkara Prabath W B
Department of Emergency Medicine Amsterdam Public Health Research Institute Amsterdam UMC, Vrije Universiteit Amsterdam Amsterdam The Netherlands.
Department of General and Acute Internal Medicine Amsterdam Public Health Research Institute Amsterdam UMC, Vrije Universiteit Amsterdam Amsterdam The Netherlands.
J Am Coll Emerg Physicians Open. 2022 May 19;3(3):e12621. doi: 10.1002/emp2.12621. eCollection 2022 Jun.
During the winter, many patients present with suspected infection that could be a viral or a bacterial (co)infection. The aim of this study is to investigate whether the optimal use of procalcitonin (PCT) is different in patients with and without proven viral infections for the purpose of excluding bacteremia. We hypothesize that when a viral infection is confirmed, this lowers the probability of bacteremia and, therefore, influences the appropriate cutoff of procalcitonin.
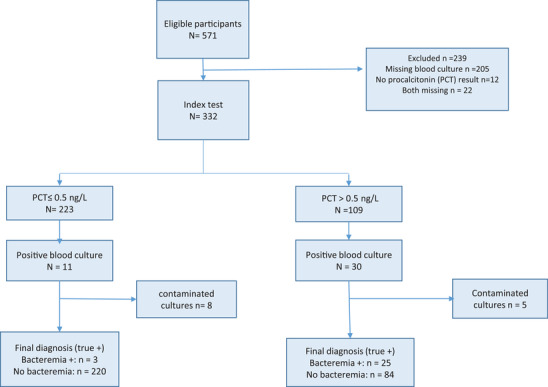
This study was conducted in the emergency department of an academic medical center in The Netherlands in the winter seasons of 2019 and 2020. Adults (>18 years) with suspected infection, in whom a blood culture and a rapid polymerase chain reaction test for influenza was performed were included.
A total of 546 patients were included of whom 47 (8.6%) had a positive blood culture. PCT had an area under the curve of 0.85, 95% confidence interval (95% CI) 0.80-0.91, for prediction of bacteremia. In patients with a proven viral infection (N = 212) PCT < 0.5 μg/L had a sensitivity of 100% (95% CI 63.1-100) and specificity of 81.2% (95% CI 75.1-86.3) to exclude bacteremia. In patients without a viral infection, the procalcitonin cutoff point of < 0.25 μg/L showed a sensitivity of 87.2% (95% CI 72.6-95.7) and specificity of 64.1 % (95% CI 58.3-69.6).
In patients with a viral infection, our findings suggest that a PCT concentration of <0.50 μg/L makes bacteremia unlikely. However, this finding needs to be confirmed in a larger population of patients with viral infections, especially because the rate of coinfection in our cohort was low.
在冬季,许多患者表现出疑似感染,可能是病毒感染或细菌(合并)感染。本研究的目的是调查在排除菌血症方面,降钙素原(PCT)在有和没有确诊病毒感染的患者中的最佳使用是否不同。我们假设,当确诊病毒感染时,这会降低菌血症的概率,因此会影响降钙素原的合适临界值。
本研究于2019年和2020年冬季在荷兰一家学术医疗中心的急诊科进行。纳入了怀疑感染且进行了血培养和流感快速聚合酶链反应检测的成年人(>18岁)。
共纳入546例患者,其中47例(8.6%)血培养呈阳性。PCT预测菌血症的曲线下面积为0.85,95%置信区间(95%CI)为0.80 - 0.91。在确诊病毒感染的患者(N = 212)中,PCT < 0.5 μg/L排除菌血症的敏感性为100%(95%CI 63.1 - 100),特异性为81.2%(95%CI 75.1 - 86.3)。在没有病毒感染的患者中,降钙素原临界值< 0.25 μg/L的敏感性为87.2%(95%CI 72.6 - 95.7),特异性为64.1%(95%CI 58.3 - 69.6)。
在病毒感染患者中,我们的研究结果表明,PCT浓度<0.50 μg/L不太可能发生菌血症。然而,这一发现需要在更大规模的病毒感染患者群体中得到证实,特别是因为我们队列中的合并感染率较低。