Lin Chiung-Tsung, Lu Jang-Jih, Chen Yu-Ching, Kok Victor C, Horng Jorng-Tzong
Department of Bioinformatics and Medical Engineering, Asia University Taiwan, Taichung, Taiwan.
Department of Laboratory Medicine, China Medical University Hospital, Taichung, Taiwan.
PeerJ. 2017 Nov 27;5:e4094. doi: 10.7717/peerj.4094. eCollection 2017.
Few studies compared the diagnostic value of procalcitonin with a combination of other tests including lactate and high-sensitivity C-reactive protein in the prediction of pathogenic bacteremia in emergency department adult patients.
We performed a retrospective study assessing the differences in performances of procalcitonin at a cutoff of 0.5 ng/mL, lactate at a cutoff of 19.8 mg/dL, high-sensitivity C-reactive protein at a cutoff of 0.8 mg/dL and their combinations for predicting bacteremia in emergency department adult patients. Sensitivity, specificity, overall accuracy, positive-test and negative-test likelihood, and diagnostic odds ratio with 95% confidence interval for each test combination were calculated for comparison. The receiver operating characteristic curve for every single test were compared using DeLong's method. We also performed a sensitivity analysis in two expanded patient cohorts to assess the discriminative ability of procalcitonin or test combination.
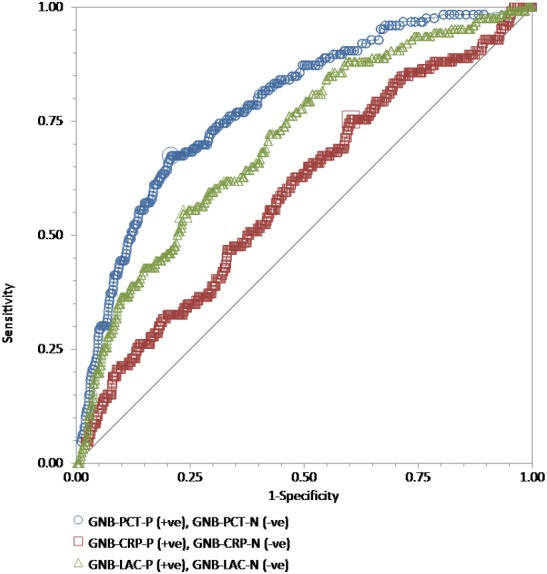
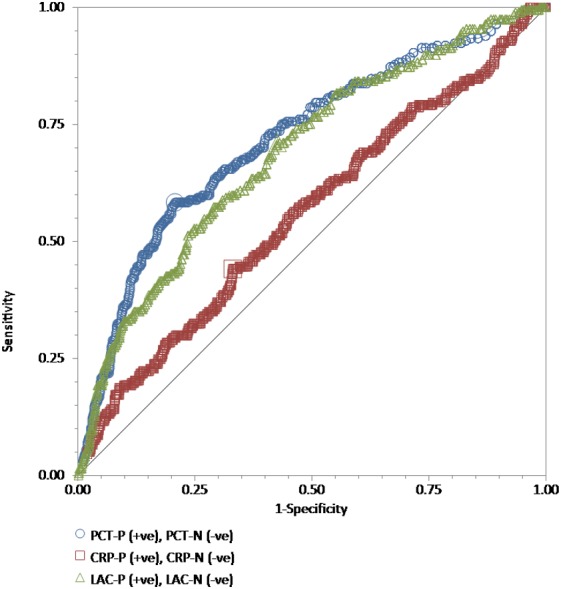
A total of 886 patients formed the initial patient cohort. The area under the receiver operating characteristic curve for discriminating positive blood culture was: procalcitonin = 0.72 (95% CI [0.69-0.75]) with a derived optimal cutoff at 3.9 ng/mL; lactate 0.69 (0.66-0.72) with an optimal cutoff at 17.9 mg/dL; high-sensitivity C-reactive protein 0.56 (0.53-0.59) with an optimal cutoff of 13 mg/dL; with pairwise comparisons showing statistically significant better performance of either procalcitonin or lactate outperforming high-sensitivity C-reactive protein. To predict positive blood cultures, the diagnostic odds ratio for procalcitonin was 3.64 (95% CI [2.46-5.51]), lactate 2.93 (2.09-4.14), and high-sensitivity C-reactive protein 0.91 (0.55-1.55; = 0.79). About combined tests, the diagnostic odds ratio for procalcitonin and lactate increases were 3.98 (95% CI [2.81-5.63]) for positive blood culture prediction. Elevated procalcitonin level rendered a six-fold increased risk of positive gram-negative bacteremia with a diagnostic odds ratio of 6.44 (95% CI [3.65-12.15]), which showed no further improvement in any test combinations. In the sensitivity analysis, as a single test to predict unspecified, gram-negative and gram-positive bacteremia, procalcitonin performed even better in an expanded cohort of 2,234 adult patients in terms of the diagnostic odds ratio.
For adult emergency patients, procalcitonin has an acceptable discriminative ability for bacterial blood culture and a better discriminative ability for gram-negative bacteremia when compared with lactate and high-sensitivity C-reactive protein. High-sensitivity C-reactive protein at a cutoff of 0.8 mg/dL performed poorly for the prediction of positive bacterial culture.
很少有研究比较降钙素原与包括乳酸和高敏C反应蛋白在内的其他检查联合使用在预测急诊科成年患者致病性菌血症方面的诊断价值。
我们进行了一项回顾性研究,评估降钙素原(截断值为0.5 ng/mL)、乳酸(截断值为19.8 mg/dL)、高敏C反应蛋白(截断值为0.8 mg/dL)及其联合检测在预测急诊科成年患者菌血症方面的性能差异。计算每个检测组合的敏感性、特异性、总体准确性、阳性检测和阴性检测似然比以及诊断比值比(95%置信区间)以进行比较。使用德龙方法比较每个单一检测的受试者工作特征曲线。我们还在两个扩大的患者队列中进行了敏感性分析,以评估降钙素原或检测组合的鉴别能力。
共有886例患者组成初始患者队列。鉴别血培养阳性的受试者工作特征曲线下面积为:降钙素原=0.72(95%置信区间[0.69 - 0.75]),推导的最佳截断值为3.9 ng/mL;乳酸0.69(0.66 - 0.72),最佳截断值为17.9 mg/dL;高敏C反应蛋白0.56(0.53 - 0.59),最佳截断值为13 mg/dL;两两比较显示降钙素原或乳酸的性能在统计学上显著优于高敏C反应蛋白。为预测血培养阳性,降钙素原的诊断比值比为3.64(95%置信区间[2.46 - 5.51]),乳酸为2.93(2.09 - 4.14),高敏C反应蛋白为0.91(0.55 - 1.55;P = 0.79)。关于联合检测,降钙素原和乳酸升高用于预测血培养阳性的诊断比值比为3.98(95%置信区间[2.81 - 5.63])。降钙素原水平升高使革兰氏阴性菌血症阳性风险增加6倍,诊断比值比为6.44(95%置信区间[3.65 - 12.15]),在任何检测组合中均未显示出进一步改善。在敏感性分析中,作为预测未指定、革兰氏阴性和革兰氏阳性菌血症的单一检测,降钙素原在一个扩大的2234例成年患者队列中,就诊断比值比而言表现更好。
对于成年急诊患者,降钙素原对细菌血培养具有可接受的鉴别能力,与乳酸和高敏C反应蛋白相比,对革兰氏阴性菌血症具有更好的鉴别能力。截断值为0.8 mg/dL的高敏C反应蛋白在预测细菌培养阳性方面表现不佳。