Zimmerman Chelsea F, Ilstad-Minnihan Alexandra B, Bruggeman Brittany S, Bruggeman Bradley J, Dayton Kristin J, Joseph Nancy, Moas Daniel I, Rohrs Henry J
Division of Pediatric Endocrinology, College of Medicine, University of Florida, Gainesville, Florida.
College of Medicine, University of Florida, Gainesville, Florida.
AACE Clin Case Rep. 2022 Jan 3;8(3):124-127. doi: 10.1016/j.aace.2021.12.005. eCollection 2022 May-Jun.
Transient thyrotoxicosis has been documented in the setting of hyperemesis gravidarum (HG) with elevated human chorionic gonadotropin (hCG) levels. Thyroid storm in pregnancy is rarer and typically associated with autoimmune hyperthyroidism. We described thyroid storm in a primigravid 18-year-old patient due to hCG level elevation secondary to HG, which resolved in the second trimester of pregnancy.
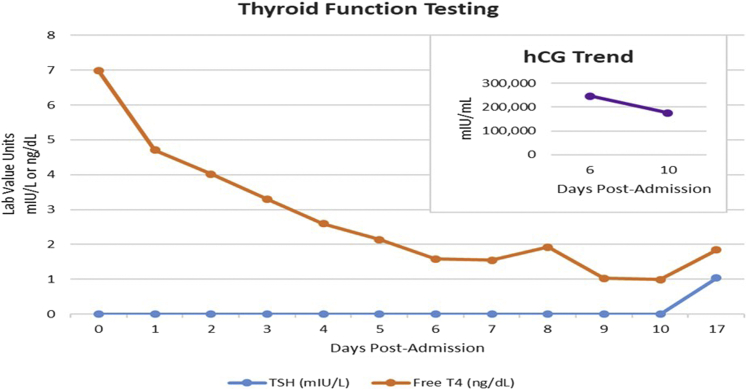
Our patient presented with vomiting, hyperthyroidism, and cardiac and renal dysfunction at 16 weeks' gestation. She was clinically found to have a thyroid storm, with undetectable thyroid-stimulating hormone (TSH) and a free thyroxine level of >6.99 ng/dL. The hCG level was elevated at 246 030 mIU/L (9040-56 451 mIU/L). She was treated with methimazole, saturated solution potassium iodide, and propranolol. Because thyroid autoantibodies were absent, thyroid ultrasound yielded normal results, and thyroid function testing results rapidly improved as the hCG level decreased, the medications were tapered and ultimately discontinued by day 10 of hospitalization. The thyroid function remained normal after discharge.
Because hCG and TSH have identical alfa subunits and similar beta subunits, hCG can bind to the TSH receptor and stimulate thyroxine production. The hCG level peaks at around 8-14 weeks of gestation, correlating with decreased TSH levels in this same time frame. This case emphasizes the relevant physiology and importance of timely and thorough evaluation to determine the appropriate management, prognosis, and follow-up for patients with thyroid storm in the setting of HG.
Although transient thyrotoxicosis is documented in patients with HG, thyroid storm is rare, and our case illustrates a severe example of these comorbidities.
在妊娠剧吐(HG)且人绒毛膜促性腺激素(hCG)水平升高的情况下,已记录到短暂性甲状腺毒症。妊娠期甲状腺风暴较为罕见,通常与自身免疫性甲状腺功能亢进有关。我们描述了一名18岁初孕妇因HG继发hCG水平升高而发生甲状腺风暴的病例,该病例在妊娠中期得到缓解。
我们的患者在妊娠16周时出现呕吐、甲状腺功能亢进以及心脏和肾功能不全。临床检查发现她患有甲状腺风暴促甲状腺激素(TSH)检测不到,游离甲状腺素水平>6.99 ng/dL。hCG水平升高至246 030 mIU/L(9040 - 56 451 mIU/L)。她接受了甲巯咪唑、饱和碘化钾溶液和普萘洛尔治疗。由于不存在甲状腺自身抗体,甲状腺超声检查结果正常,且随着hCG水平下降甲状腺功能测试结果迅速改善,药物逐渐减量,最终在住院第10天停药。出院后甲状腺功能保持正常。
由于hCG和TSH具有相同的α亚基和相似的β亚基,hCG可与TSH受体结合并刺激甲状腺素生成。hCG水平在妊娠8 - 14周左右达到峰值,与此期间TSH水平下降相关。该病例强调了相关生理学以及及时、全面评估对于确定HG背景下甲状腺风暴患者适当治疗、预后和随访的重要性。
尽管HG患者中记录到短暂性甲状腺毒症,但甲状腺风暴罕见,我们的病例说明了这些合并症的一个严重实例。