Gastrointestinal Cancer Center, Dana-Farber Cancer Institute, Boston, MA, USA.
Department of Health Science Research, Mayo Clinic, Rochester, MN, USA.
JNCI Cancer Spectr. 2022 Mar 2;6(2). doi: 10.1093/jncics/pkac014.
We evaluated the time to progression (TTP) and survival outcomes of second-line therapy for metastatic colorectal cancer among adults aged 70 years and older compared with younger adults following progression on first-line clinical trials.
Associations between clinical and disease characteristics, time to initial progression, and rate of receipt of second-line therapy were evaluated. TTP and overall survival (OS) were compared between older and younger adults in first- and second-line trials by Cox regression, adjusting for age, sex, Eastern Cooperative Oncology Group Performance Status, number of metastatic sites and presence of metastasis in the lung, liver, or peritoneum. All statistical tests were 2-sided.
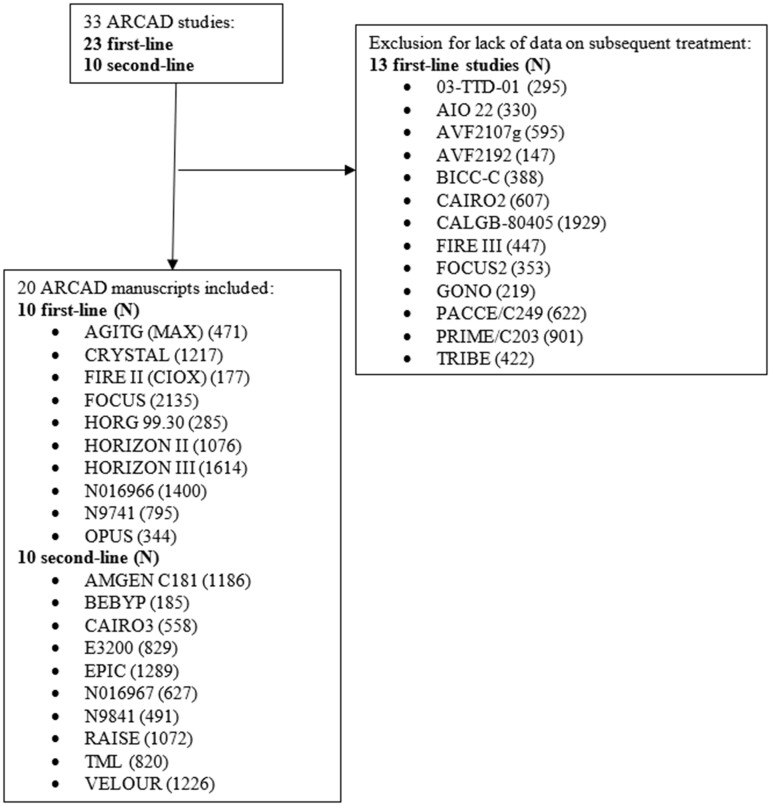
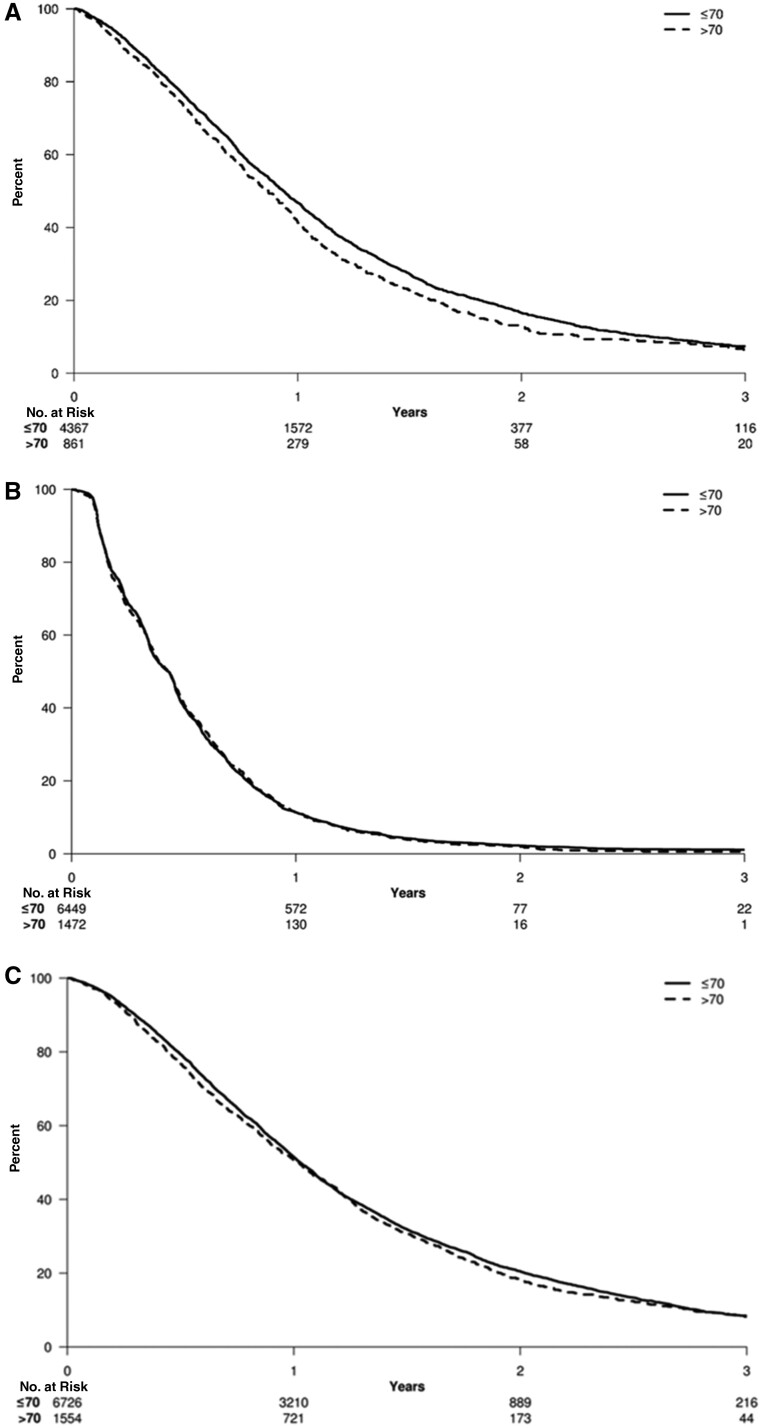
Older adults comprised 16.4% of patients on first-line trials (870 total older adults aged >70 years; 4419 total younger adults aged ≤70 years, on first-line trials). Older adults and those with Eastern Cooperative Oncology Group Performance Status >0 were less likely to receive second-line therapy than younger adults. Odds of receiving second-line therapy decreased by 11% for each additional decade of life in multivariable analysis (odds ratio = 1.11, 95% confidence interval = 1.02 to 1.21, P = .01). Older and younger adults enrolled in second-line trials experienced similar median TTP and median OS (median TTP = 5.1 vs 5.2 months, respectively; median OS = 11.6 vs 12.4 months, respectively).
Older adults were less likely to receive second-line therapy for metastatic colorectal cancer, though we did not observe a statistical difference in survival outcomes vs younger adults following second-line therapy. Further study should examine factors affecting decisions to treat older adults with second-line therapy. Inclusion of geriatric assessment may provide better criteria regarding the risks and benefits of second-line therapy.
我们评估了一线临床试验进展后,与年轻患者相比,70 岁及以上转移性结直肠癌患者二线治疗的无进展生存期(TTP)和生存结局。
评估了临床和疾病特征、首次进展时间以及二线治疗的接受率之间的关联。通过 Cox 回归比较了一线和二线试验中年龄较大和年龄较小的成年人的 TTP 和总生存期(OS),并调整了年龄、性别、东部肿瘤协作组表现状态、转移性部位的数量以及肺、肝或腹膜转移的存在。所有统计检验均为双侧。
一线试验中 16.4%的患者为年龄较大的成年人(870 名年龄>70 岁的患者;4419 名年龄≤70 岁的患者,一线试验)。与年轻患者相比,年龄较大的患者和东部肿瘤协作组表现状态>0 的患者接受二线治疗的可能性较小。多变量分析显示,每增加十年的寿命,接受二线治疗的可能性降低 11%(优势比=1.11,95%置信区间=1.02 至 1.21,P=0.01)。参加二线试验的年龄较大和年龄较小的成年人的 TTP 和 OS 中位数相似(中位数 TTP=5.1 个月 vs 5.2 个月,中位数 OS=11.6 个月 vs 12.4 个月)。
尽管在接受二线治疗后,年龄较大的成年人与年轻成年人相比,生存结局无统计学差异,但年龄较大的成年人接受二线治疗的可能性较小。进一步的研究应该研究影响对年龄较大的成年人用二线治疗的因素。纳入老年评估可能为二线治疗的风险和益处提供更好的标准。