Department of Cardiology (CVK) and Berlin Institute of Health Center for Regenerative Therapies (BCRT); German Centre for Cardiovascular Research (DZHK) partner site Berlin; Charité Universitätsmedizin Berlin, Berlin, Germany.
Institute of Heart Diseases, Wrocław Medical University, Wrocław, Poland.
Eur J Heart Fail. 2022 Aug;24(8):1400-1405. doi: 10.1002/ejhf.2558. Epub 2022 Jun 5.
To report data from EMPEROR-Preserved according to prespecified endpoints of DELIVER.
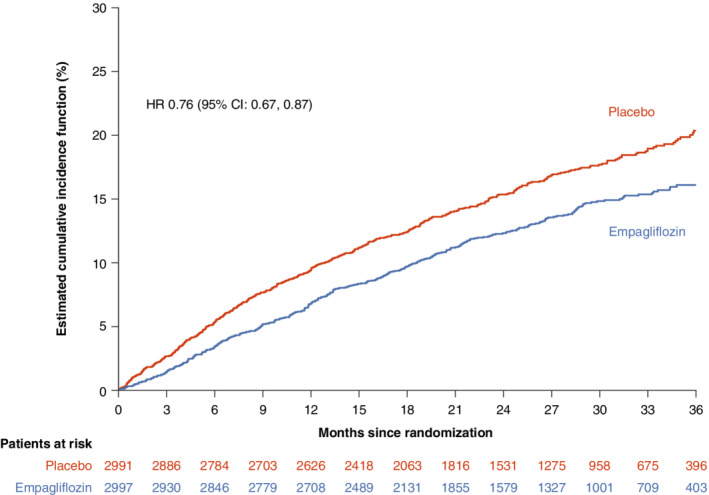
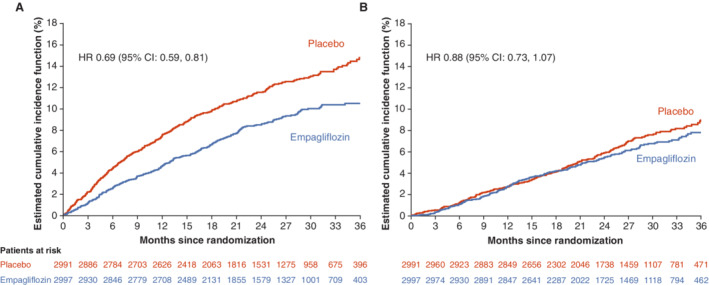
In order to assess the impact of DELIVER-like definition on EMPEROR-Preserved outcomes, the following differences were reconciled: (1) the primary outcome in DELIVER added urgent heart failure (HF) visits to cardiovascular death or HF hospitalizations; (2) the EMPEROR-Preserved trial did not require documentation of physical findings or laboratory tests for confirming a HF hospitalization and it included events of 12-24 h if intensification of treatment was not only oral diuretics; (3) DELIVER excluded undetermined causes of deaths from the primary endpoint; (4) the composite renal endpoint in DELIVER included a sustained ≥50% decline in estimated glomerular filtration rate and incorporated renal death; and (5) DELIVER will assess outcomes in the overall population and in patients with ejection fraction (EF) <60% separately. Using the endpoint definitions from DELIVER, the primary outcome overall occurred in 13.1% in the empagliflozin and 16.8% in the placebo group (hazard ratio [HR] 0.76, 95% confidence interval [CI] 0.67-0.87; p < 0.0001). The relative risk reduction (RRR) changed from 21% to 24% when urgent HF visits were added, and undetermined death was eliminated. Compared to overall population RRR of 24%, it was 28% in patients with EF <60%. Death from cardiovascular causes excluding undetermined causes occurred in 6.2% in the empagliflozin and in 7.1% in the placebo group (HR 0.88, 95% CI 0.73-1.07). The RRR for the composite renal endpoint changed from 22% in the overall population (HR 0.78, 95% CI 0.54-1.13) to 40% when patients with EF <60% were assessed (p = 0.037).
Findings from EMPEROR-Preserved were modestly altered when analysed using cardiovascular trial endpoint definitions of the DELIVER trial. For the composite renal endpoint, the effect of empagliflozin became statistically significant in patients with EF <60% using the DELIVER definition.
根据 DELIVER 的预设终点报告 EMPEROR-Preserved 的数据。
为了评估 DELIVER 样定义对 EMPEROR-Preserved 结局的影响,对以下差异进行了协调:(1)DELIVER 中的主要结局增加了紧急心力衰竭(HF)就诊,以取代心血管死亡或 HF 住院;(2)EMPEROR-Preserved 试验不需要记录物理发现或实验室检查来确认 HF 住院,并且如果强化治疗不仅是口服利尿剂,则包括 12-24 小时的事件;(3)DELIVER 从主要终点排除了未确定原因的死亡;(4)DELIVER 的复合肾脏终点包括估计肾小球滤过率持续下降≥50%,并纳入了肾脏死亡;(5)DELIVER 将分别评估整体人群和射血分数(EF)<60%的患者的结局。使用 DELIVER 的终点定义,在依帕列净组和安慰剂组中,总体主要结局分别发生在 13.1%和 16.8%(风险比[HR]0.76,95%置信区间[CI]0.67-0.87;p<0.0001)。当紧急 HF 就诊增加时,相对风险降低(RRR)从 21%变为 24%,并且消除了未确定的死亡。与整体人群的 RRR 为 24%相比,EF<60%的患者为 28%。心血管原因导致的死亡,不包括未确定原因的死亡,在依帕列净组中发生了 6.2%,在安慰剂组中发生了 7.1%(HR 0.88,95%CI 0.73-1.07)。复合肾脏终点的 RRR 从整体人群的 22%(HR 0.78,95%CI 0.54-1.13)变化为 EF<60%患者评估时的 40%(p=0.037)。
当使用 DELIVER 试验的心血管试验终点定义分析 EMPEROR-Preserved 的结果时,发现结果略有改变。对于复合肾脏终点,使用 DELIVER 定义时,EF<60%的患者依帕列净的效果具有统计学意义。