T1D Exchange, QI & Population Health Department, Boston, Massachusetts, USA.
Stanford University, Division of Pediatric Endocrinology & Diabetes, Lucile Packard Children's Hospital, Stanford, California, USA.
Diabetes Technol Ther. 2022 Sep;24(9):619-627. doi: 10.1089/dia.2022.0042. Epub 2022 Jun 13.
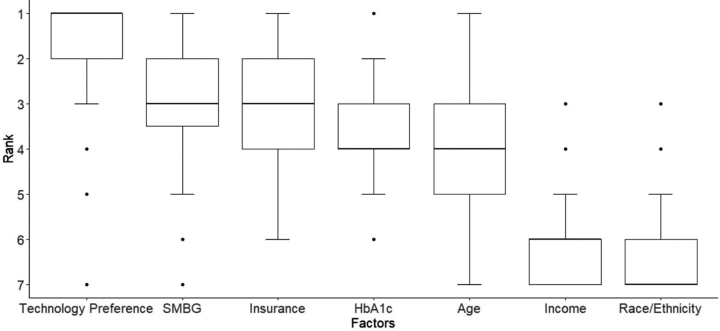
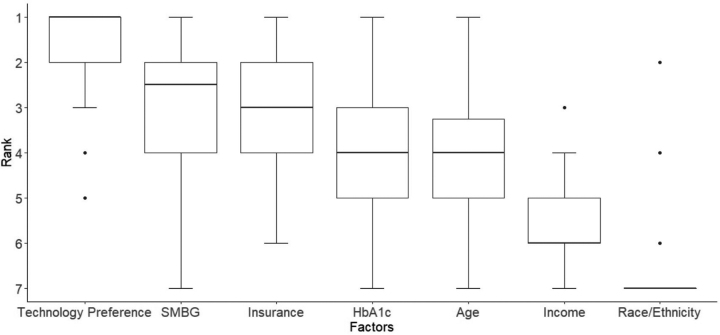
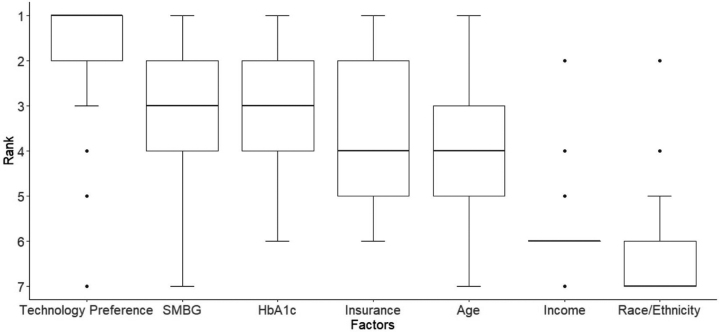
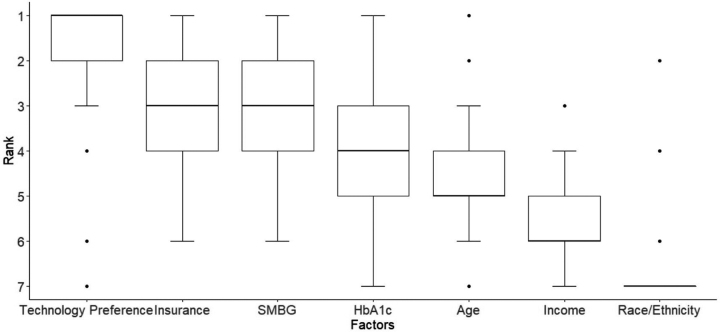
Despite documented benefits of diabetes technology in managing type 1 diabetes, inequities persist in the use of these devices. Provider bias may be a driver of inequities, but the evidence is limited. Therefore, we aimed to examine the role of race/ethnicity and insurance-mediated provider implicit bias in recommending diabetes technology. We recruited 109 adult and pediatric diabetes providers across 7 U.S. endocrinology centers to complete an implicit bias assessment composed of a clinical vignette and ranking exercise. Providers were randomized to receive clinical vignettes with differing insurance and patient names as proxy for Racial-Ethnic identity. Bias was identified if providers: (1) recommended more technology for patients with an English name (Racial-Ethnic bias) or private insurance (insurance bias), or (2) Race/Ethnicity or insurance was ranked high (Racial-Ethnic and insurance bias, respectively) in recommending diabetes technology. Provider characteristics were analyzed using descriptive statistics and multivariate logistic regression. Insurance-mediated implicit bias was common in our cohort ( = 66, 61%). Providers who were identified to have insurance-mediated bias had greater years in practice (5.3 ± 5.3 years vs. 9.3 ± 9 years, = 0.006). Racial-Ethnic-mediated implicit bias was also observed in our study ( = 37, 34%). Compared with those without Racial-Ethnic bias, providers with Racial-Ethnic bias were more likely to state that they could recognize their own implicit bias (89% vs. 61%, = 0.001). Provider implicit bias to recommend diabetes technology was observed based on insurance and Race/Ethnicity in our pediatric and adult diabetes provider cohort. These data raise the need to address provider implicit bias in diabetes care.
尽管有文献证明糖尿病技术在管理 1 型糖尿病方面的益处,但在这些设备的使用方面仍存在不平等现象。医生的偏见可能是造成不平等的一个因素,但证据有限。因此,我们旨在研究种族/民族和保险中介的提供者内隐偏见在推荐糖尿病技术方面的作用。我们招募了美国 7 个内分泌中心的 109 名成人和儿科糖尿病医生,让他们完成了一项内隐偏见评估,包括一个临床案例和排名练习。医生被随机分配到不同的保险和患者姓名的临床案例中,作为种族/民族身份的代理。如果提供者:(1) 更推荐有英文名字的患者使用技术(种族/民族偏见)或私人保险(保险偏见),或者 (2) 在推荐糖尿病技术时将种族/民族或保险列为首位(分别为种族/民族和保险偏见),则认为存在偏见。使用描述性统计和多元逻辑回归分析提供者特征。我们的队列中存在常见的保险中介内隐偏见( = 66, 61%)。被认为存在保险中介偏见的医生,其行医年限更长(5.3±5.3 年比 9.3±9 年, = 0.006)。我们的研究也观察到了种族/民族中介的内隐偏见( = 37, 34%)。与没有种族/民族偏见的医生相比,有偏见的医生更有可能表示他们可以认识到自己的内隐偏见(89%比 61%, = 0.001)。在我们的儿科和成人糖尿病医生队列中,根据保险和种族/民族,观察到医生推荐糖尿病技术的内隐偏见。这些数据提出了在糖尿病护理中解决提供者内隐偏见的需要。