Department of Surgery, Erasmus University Medical Centre, Rotterdam, The Netherlands.
Department of Surgery, Erasmus University Medical Center, Wytemaweg 80 3015 CN Room Ee-173, Rotterdam, The Netherlands.
Surg Endosc. 2022 Oct;36(10):7764-7774. doi: 10.1007/s00464-022-09326-3. Epub 2022 May 23.
This study aimed to compare laparoscopic lavage and sigmoidectomy as treatment for perforated diverticulitis with purulent peritonitis during a 36 month follow-up of the LOLA trial.
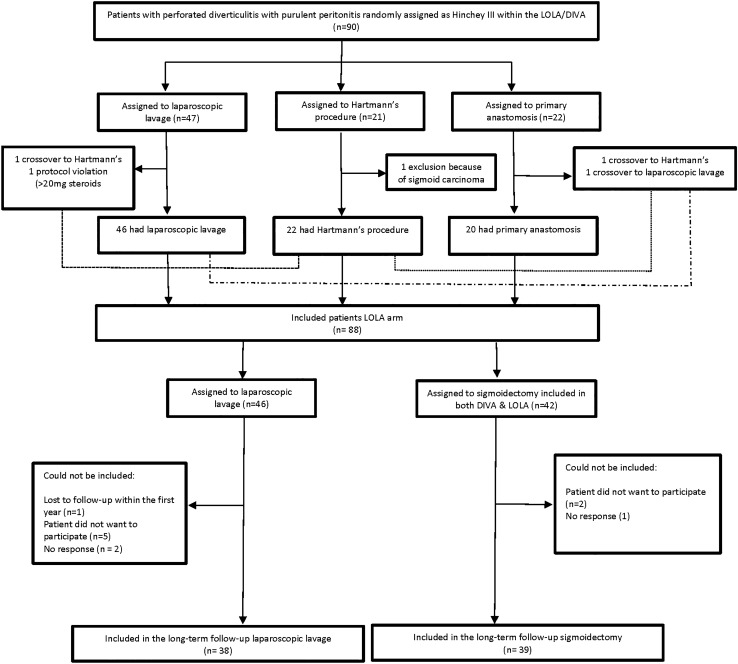
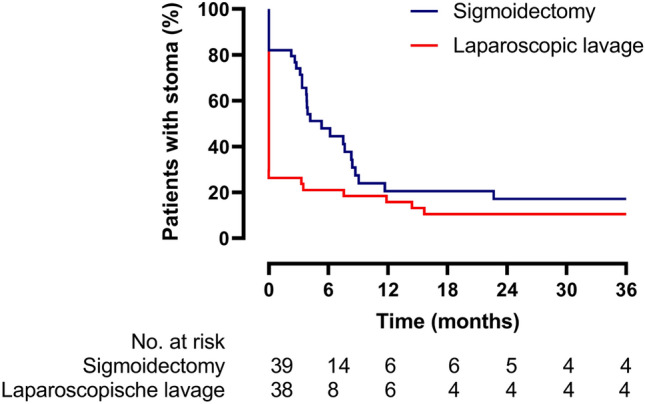
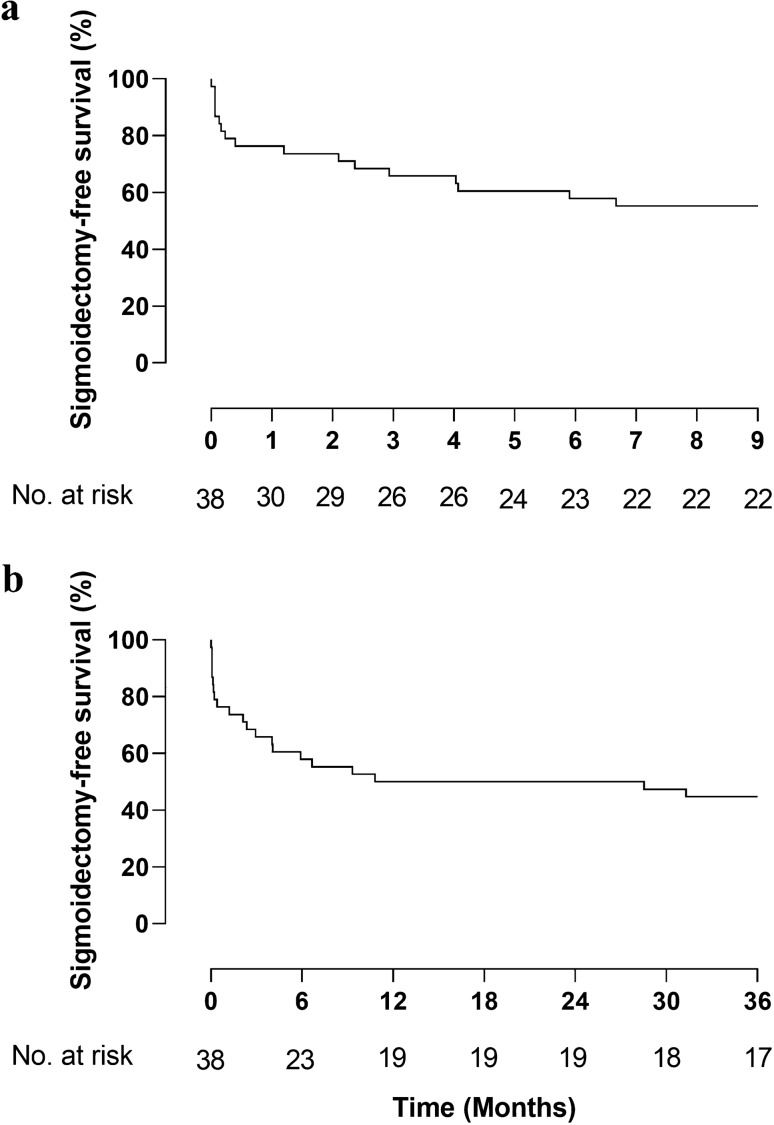
Within the LOLA arm of the international, multicentre LADIES trial, patients with perforated diverticulitis with purulent peritonitis were randomised between laparoscopic lavage and sigmoidectomy. Outcomes were collected up to 36 months. The primary outcome of the present study was cumulative morbidity and mortality. Secondary outcomes included reoperations (including stoma reversals), stoma rates, and sigmoidectomy rates in the lavage group.
Long-term follow-up was recorded in 77 of the 88 originally included patients, 39 were randomised to sigmoidectomy (51%) and 38 to laparoscopic lavage (49%). After 36 months, overall cumulative morbidity (sigmoidectomy 28/39 (72%) versus lavage 32/38 (84%), p = 0·272) and mortality (sigmoidectomy 7/39 (18%) versus lavage 6/38 (16%), p = 1·000) did not differ. The number of patients who underwent a reoperation was significantly lower for lavage compared to sigmoidectomy (sigmoidectomy 27/39 (69%) versus lavage 17/38 (45%), p = 0·039). After 36 months, patients alive with stoma in situ was lower in the lavage group (proportion calculated from the Kaplan-Meier life table, sigmoidectomy 17% vs lavage 11%, log-rank p = 0·0268). Eventually, 17 of 38 (45%) patients allocated to lavage underwent sigmoidectomy.
Long-term outcomes showed that laparoscopic lavage was associated with less patients who underwent reoperations and lower stoma rates in patients alive after 36 months compared to sigmoidectomy. No differences were found in terms of cumulative morbidity or mortality. Patient selection should be improved to reduce risk for short-term complications after which lavage could still be a valuable treatment option.
本研究旨在通过 LOLA 试验 36 个月的随访,比较腹腔镜灌洗和乙状结肠切除术治疗伴有脓性腹膜炎的穿孔性憩室炎。
在国际多中心 LADIES 试验的 LOLA 臂中,对伴有脓性腹膜炎的穿孔性憩室炎患者进行腹腔镜灌洗和乙状结肠切除术的随机分组。结果随访至 36 个月。本研究的主要结局是累积发病率和死亡率。次要结局包括再手术(包括造口反转)、造口率和灌洗组的乙状结肠切除术率。
88 例最初纳入患者中有 77 例记录了长期随访结果,其中 39 例随机分为乙状结肠切除术(51%),38 例随机分为腹腔镜灌洗组(49%)。36 个月后,总体累积发病率(乙状结肠切除术 28/39(72%)与灌洗组 32/38(84%),p=0.272)和死亡率(乙状结肠切除术 7/39(18%)与灌洗组 6/38(16%),p=1.000)无差异。与乙状结肠切除术相比,灌洗组行再手术的患者明显减少(乙状结肠切除术 27/39(69%)与灌洗组 17/38(45%),p=0.039)。36 个月后,灌洗组仍有造口的患者比例较低(根据 Kaplan-Meier 生命表计算的比例,乙状结肠切除术组为 17%,灌洗组为 11%,log-rank p=0.0268)。最终,38 例中有 17 例(45%)被分配到灌洗组的患者接受了乙状结肠切除术。
长期结果表明,与乙状结肠切除术相比,腹腔镜灌洗在 36 个月后再手术患者比例和有造口的患者比例较低,而累积发病率或死亡率无差异。应该改善患者选择,以降低短期并发症的风险,此后灌洗仍然是一种有价值的治疗选择。