Department of Medical Diagnostics, Faculty of Allied Health Sciences, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana.
Department of Molecular Medicine, School of Medicine and Dentistry, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana.
AIDS Res Ther. 2022 May 25;19(1):21. doi: 10.1186/s12981-022-00447-2.
Viral suppression remains the most desired outcome in the management of patients with Human Immunodeficiency Virus/Acquired Immune Deficiency Syndrome (HIV/AIDS) and this can be achieved by an effective Antiretroviral Therapy (ART). However, some patients who achieve viral suppression may experience viral rebound with dire consequence. We evaluated viral suppression and rebound and their associated factors among adult patients on ART in Kumasi, Ghana.
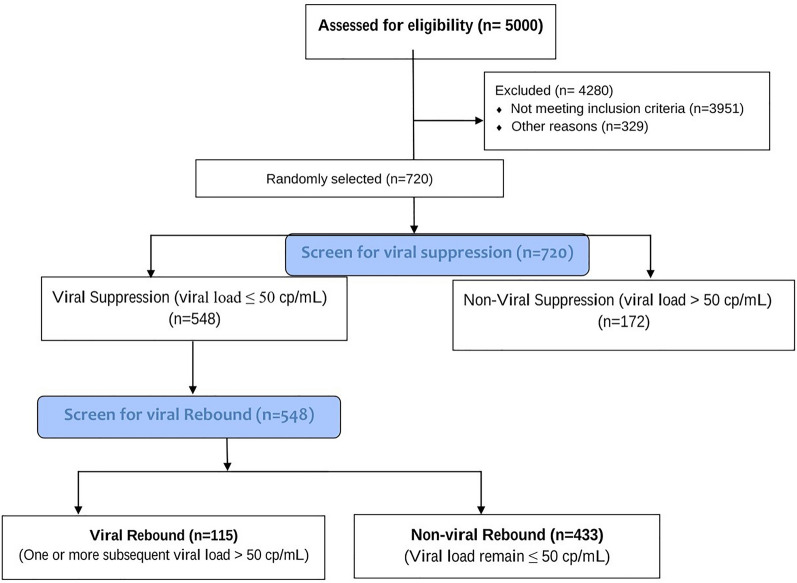
This hospital-based retrospective study was conducted at the Komfo Anokye Teaching Hospital in Ghana. We reviewed the medical records of 720 HIV patients on ART. Statistical analyses were performed using SPSS Version 26.0 and GraphPad prism version 8.0. p < 0.05 was considered statistically significant.
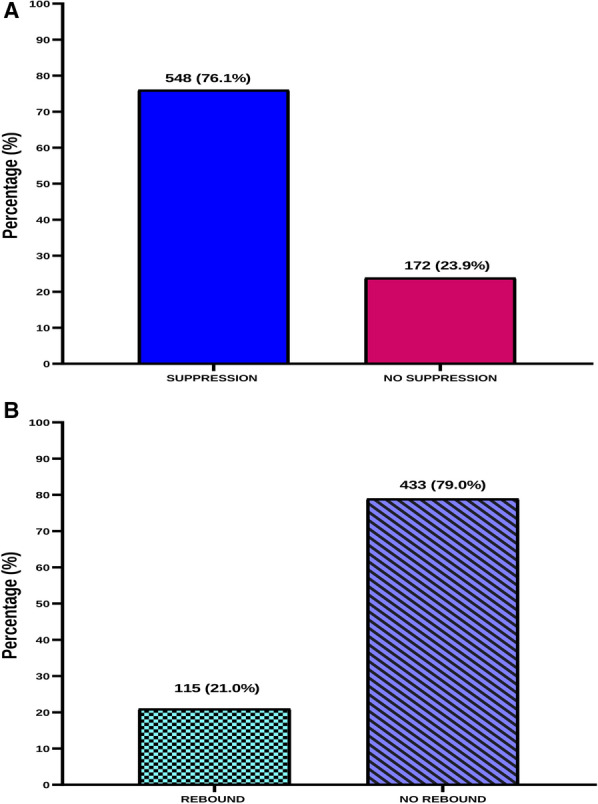
Proportions of patients with viral suppression and viral rebound were 76.1% and 21.0% respectively. Being diagnosed at WHO stage I [aOR = 11.40, 95% CI (3.54-36.74), p < 0.0001], having good adherence to ART [aOR = 5.09, 95% CI (2.67-9.73), p < 0.0001], taking Nevirapine-based regimen [aOR = 4.66, 95% CI (1.20-18.04), p = 0.0260] and increasing duration of treatment (p < 0.0001) were independently associated with higher odds of viral suppression. However, being diagnosed at WHO stage II (aOR = 7.39, 95% CI 2.67-20.51; p < 0.0001) and stage III (aOR = 8.62, 95% CI 3.16-23.50; p < 0.0001), having poor adherence (aOR = 175.48, 95% CI 44.30-695.07; p < 0.0001), recording baseline suppression value of 20-49 copies/mL (aOR = 6.43, 95% CI 2.72-15.17; p < 0.0001) and being treated with Zidovudine/Lamivudine/Efavirenz (aOR = 6.49, 95% CI 1.85-22.79; p = 0.004) and Zidovudine/Lamivudine/Nevirapine (aOR = 18.68, 95% CI 1.58-220.90; p = 0.02) were independently associated with higher odds of viral rebound.
Approximately 76% viral suppression rate among HIV patients on ART in Kumasi falls below the WHO 95% target by the year 2030. Choice of ART combination, drug adherence, WHO clinical staging and baseline viral load are factors associated with suppression or rebound. These clinical characteristics of HIV patients must be monitored concurrently with the viral load.
在人类免疫缺陷病毒/获得性免疫缺陷综合征(HIV/AIDS)患者的管理中,病毒抑制仍然是最理想的结果,这可以通过有效的抗逆转录病毒疗法(ART)来实现。然而,一些达到病毒抑制的患者可能会出现病毒反弹,导致严重后果。我们评估了加纳库马西接受 ART 的成年患者的病毒抑制和反弹及其相关因素。
这是一项在加纳科福·阿肯耶教学医院进行的基于医院的回顾性研究。我们回顾了 720 名接受 ART 的 HIV 患者的病历。使用 SPSS 版本 26.0 和 GraphPad prism 版本 8.0 进行统计分析。p<0.05 被认为具有统计学意义。
病毒抑制和病毒反弹的患者比例分别为 76.1%和 21.0%。被诊断为世界卫生组织(WHO)阶段 I(优势比[aOR] = 11.40,95%置信区间[CI](3.54-36.74),p<0.0001)、具有良好的 ART 依从性(aOR = 5.09,95%CI(2.67-9.73),p<0.0001)、使用奈韦拉平为基础的方案(aOR = 4.66,95%CI(1.20-18.04),p=0.0260)和治疗持续时间延长(p<0.0001)与病毒抑制的可能性更高独立相关。然而,被诊断为 WHO 阶段 II(aOR = 7.39,95%CI 2.67-20.51;p<0.0001)和阶段 III(aOR = 8.62,95%CI 3.16-23.50;p<0.0001)、依从性差(aOR = 175.48,95%CI 44.30-695.07;p<0.0001)、基线抑制值为 20-49 拷贝/mL(aOR = 6.43,95%CI 2.72-15.17;p<0.0001)和接受齐多夫定/拉米夫定/依非韦伦(aOR = 6.49,95%CI 1.85-22.79;p=0.004)和齐多夫定/拉米夫定/奈韦拉平(aOR = 18.68,95%CI 1.58-220.90;p=0.02)与病毒反弹的可能性更高独立相关。
在库马西接受 ART 的 HIV 患者中,约 76%的病毒抑制率低于世界卫生组织 2030 年 95%的目标。ART 组合的选择、药物依从性、世界卫生组织临床分期和基线病毒载量是与抑制或反弹相关的因素。必须同时监测 HIV 患者的这些临床特征和病毒载量。