Department of Intensive Care Medicine, Inselspital, Bern University Hospital, CH-3010, Bern, Switzerland.
Division of Anaesthesiology, Intensive Care, Rescue and Pain Medicine, Kantonsspital St. Gallen, St. Gallen, Switzerland.
Acta Neurochir (Wien). 2022 Jul;164(7):1805-1814. doi: 10.1007/s00701-022-05256-0. Epub 2022 May 26.
There is increasing evidence that inflammation plays a role in the pathogenesis of aneurysmal subarachnoid hemorrhage (aSAH) and in the development of delayed cerebral ischemia (DCI). However, the assessment and interpretation of classically defined inflammatory parameters is difficult in aSAH patients. The objective of this study was to investigate the relationship between easily assessable findings (hyperventilation, fever, white blood cell count (WBC), and C-reactive protein (CRP)) and the occurrence of DCI and unfavorable neurological outcome at discharge in aSAH patients.
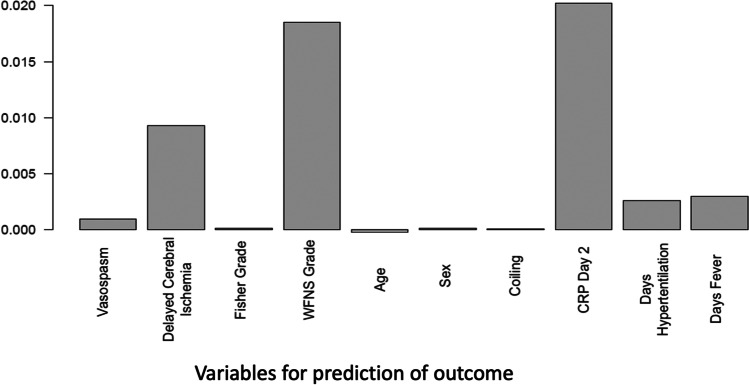
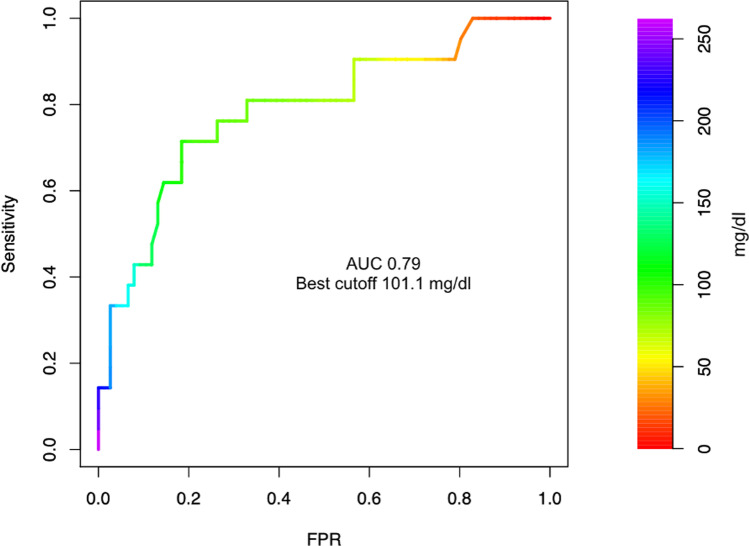
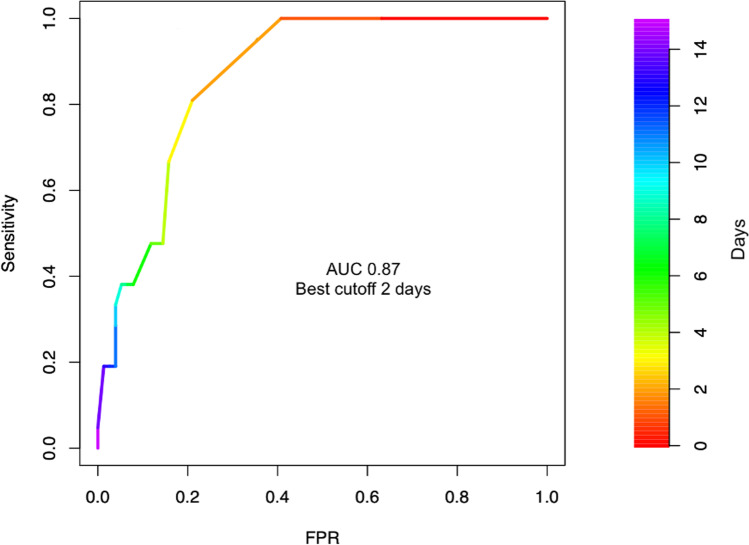
Retrospective analysis of prospectively collected data from a single center cohort. We evaluated the potential of clinical signs of inflammation (hyperventilation, fever) and simple inflammatory laboratory parameters CRP and WBC to predict unfavorable outcomes at discharge and DCI in a multivariate analysis. A cutoff value for CRP was calculated by Youden's J statistic. Outcome was measured using the modified Rankin score at discharge, with an unfavorable outcome defined as modified Rankin scale (mRS) > 3.
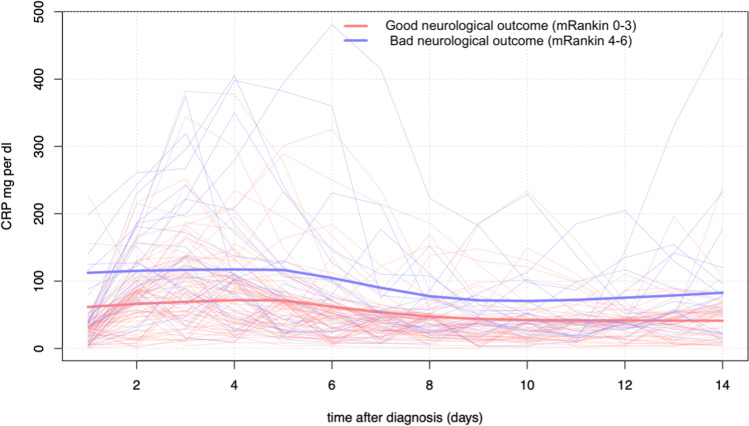
We included 97 consecutive aSAH patients (63 females, 34 males, mean age 58 years) in the analysis. Twenty-one (22%) had major disability or died by the time of hospital discharge. Among inflammatory parameters, CRP over 100 mg/dl on day 2 was an independent predictor for worse neurological outcome at discharge. The average C-reactive protein level in the first 14 days was higher in patients with a worse neurological outcome (96.6, SD 48.3 vs 56.3 mg/dl, SD 28.6) in the first 14 days after aSAH. C-reactive protein on day 2 was an indicator of worse neurological outcome. No inflammatory parameter was an independent predictor of DCI. After multivariate adjustment, DCI, increased age, and more than 1 day of mechanical ventilation were significant predictors of worse neurological outcome.
Early elevated CRP levels were a significant predictor of worse neurological outcome at hospital discharge and may be a useful marker of later deterioration in aSAH.
越来越多的证据表明,炎症在动脉瘤性蛛网膜下腔出血(aSAH)的发病机制和迟发性脑缺血(DCI)的发展中起作用。然而,在 aSAH 患者中,经典定义的炎症参数的评估和解释较为困难。本研究的目的是探讨在 aSAH 患者中,容易评估的发现(过度通气、发热、白细胞计数(WBC)和 C 反应蛋白(CRP))与 DCI 的发生以及出院时不良神经结局之间的关系。
回顾性分析单中心队列前瞻性收集的数据。我们通过多变量分析评估炎症的临床征象(过度通气、发热)和简单的炎症实验室参数 CRP 和 WBC 预测出院时不良结局和 DCI 的可能性。通过 Youden's J 统计计算 CRP 的临界值。使用出院时改良Rankin 评分(mRS)来衡量结局,mRS 评分大于 3 定义为不良结局。
我们纳入了 97 例连续的 aSAH 患者(63 名女性,34 名男性,平均年龄 58 岁)进行分析。21 例(22%)在出院时出现严重残疾或死亡。在炎症参数中,第 2 天 CRP 超过 100mg/dl 是出院时神经功能恶化的独立预测因素。aSAH 后第 14 天,神经功能恶化患者的平均 CRP 水平较高(96.6,SD 48.3 vs 56.3mg/dl,SD 28.6)。第 2 天的 C 反应蛋白是神经功能恶化的指标。没有炎症参数是 DCI 的独立预测因素。在多变量调整后,DCI、年龄增加和机械通气超过 1 天是神经功能恶化的显著预测因素。
早期 CRP 水平升高是出院时神经功能恶化的显著预测因素,可能是 aSAH 后病情恶化的有用标志物。