Oltmer Jan, Slepneva Natalya, Llamas Rodriguez Josue, Greve Douglas N, Williams Emily M, Wang Ruopeng, Champion Samantha N, Lang-Orsini Melanie, Nestor Kimberly, Fernandez-Ros Nídia, Fischl Bruce, Frosch Matthew P, Magnain Caroline, van der Kouwe Andre J W, Augustinack Jean C
Department of Radiology, Athinoula A. Martinos Center, Massachusetts General Hospital, Charlestown, MA, USA.
Harvard Medical School, Boston, MA, USA.
Brain Commun. 2022 Mar 25;4(3):fcac074. doi: 10.1093/braincomms/fcac074. eCollection 2022.
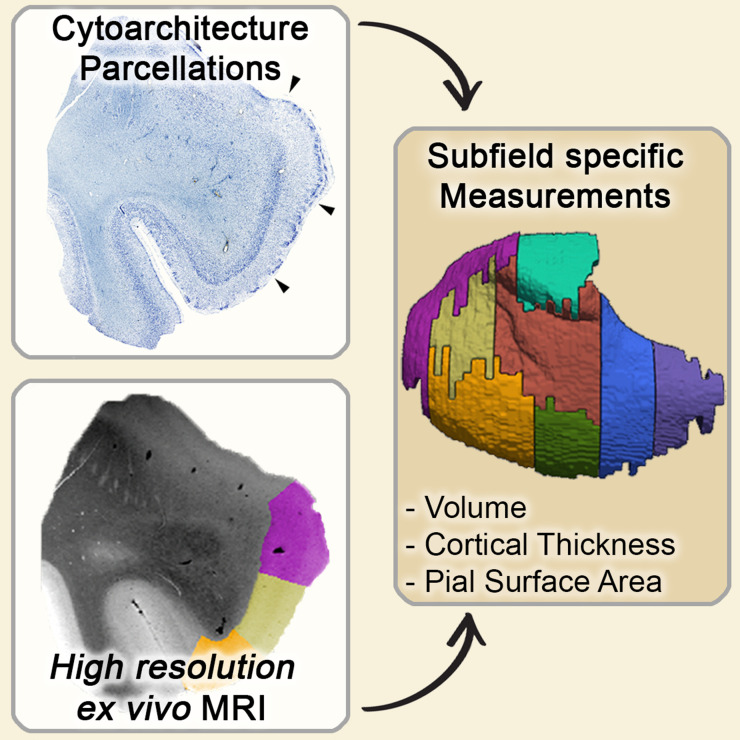
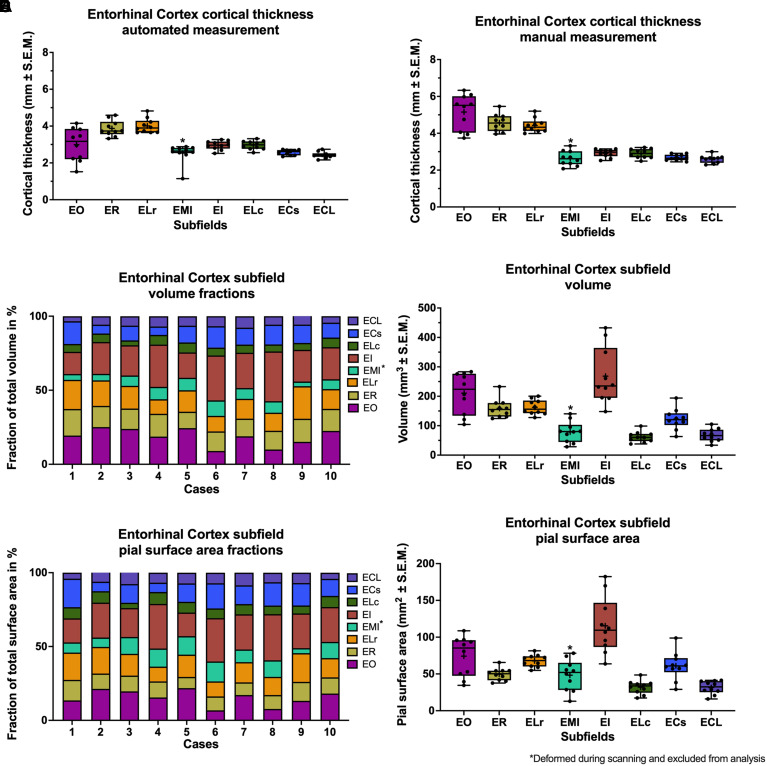
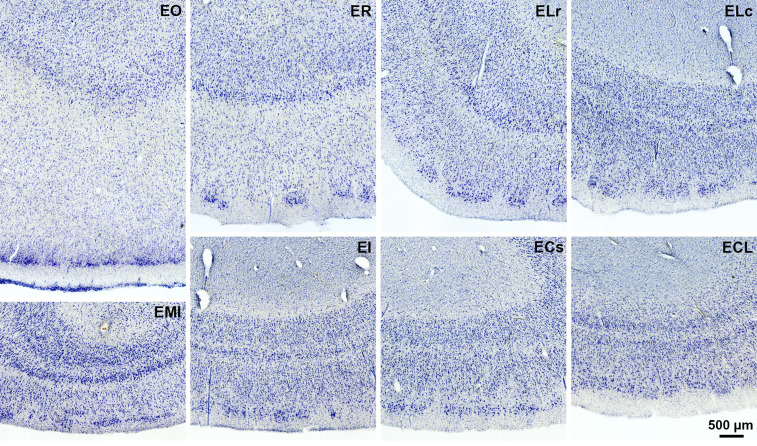
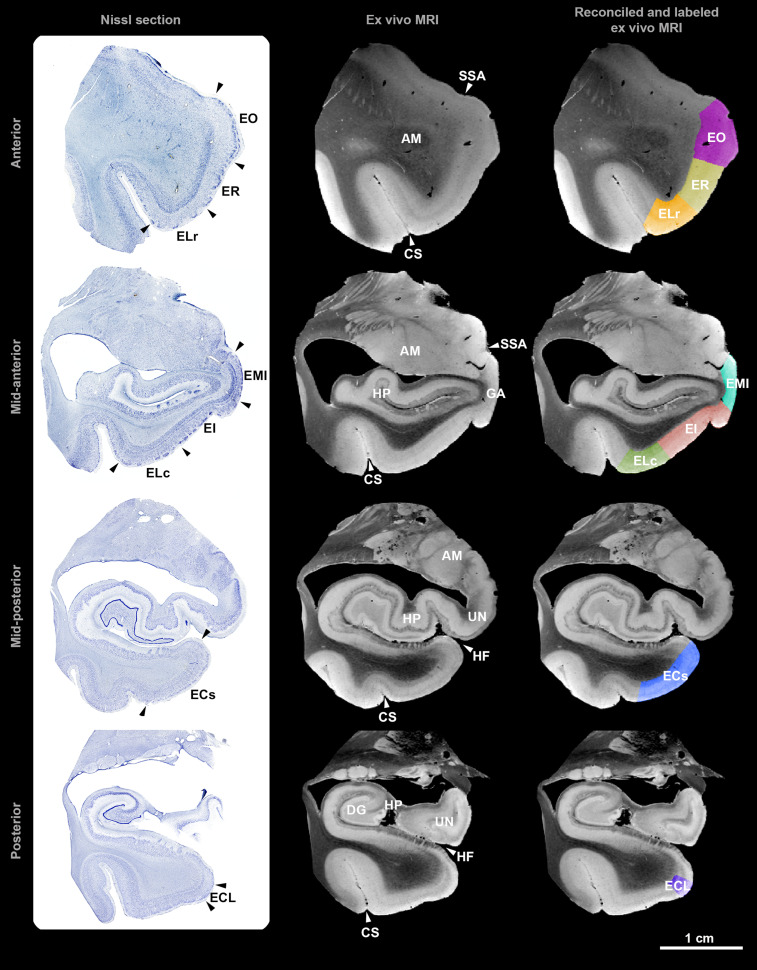
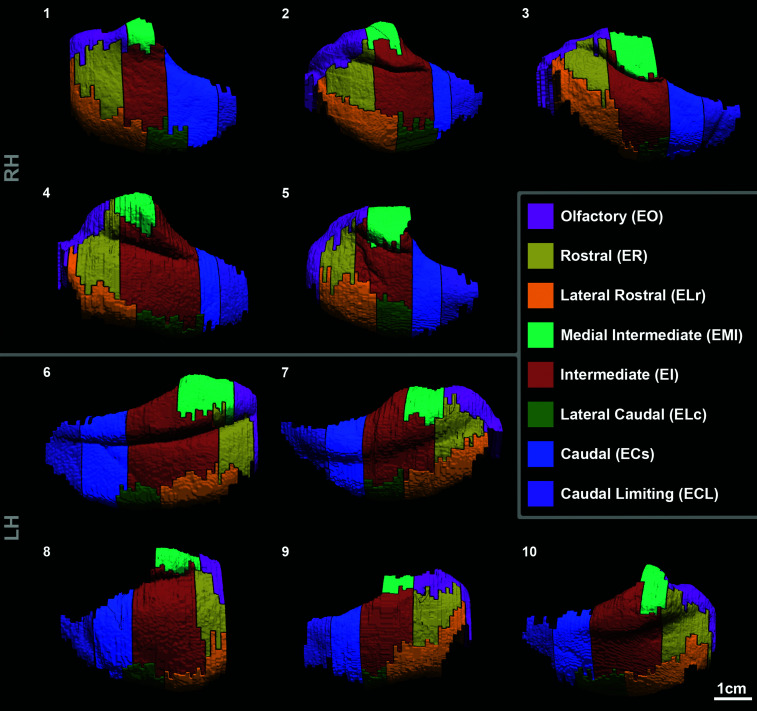
Neuroimaging studies have routinely used hippocampal volume as a measure of Alzheimer's disease severity, but hippocampal changes occur too late in the disease process for potential therapies to be effective. The entorhinal cortex is one of the first cortical areas affected by Alzheimer's disease; its neurons are especially vulnerable to neurofibrillary tangles. Entorhinal atrophy also relates to the conversion from non-clinical to clinical Alzheimer's disease. In neuroimaging, the human entorhinal cortex has so far mostly been considered in its entirety or divided into a medial and a lateral region. Cytoarchitectonic differences provide the opportunity for subfield parcellation. We investigated the entorhinal cortex on a subfield-specific level-at a critical time point of Alzheimer's disease progression. While MRI allows multidimensional quantitative measurements, only histology provides enough accuracy to determine subfield boundaries-the pre-requisite for quantitative measurements the entorhinal cortex. This study used histological data to validate ultra-high-resolution 7 Tesla MRI and create entorhinal subfield parcellations in a total of 10 pre-clinical Alzheimer's disease and normal control cases. Using MRI, eight entorhinal subfields (olfactory, rostral, medial intermediate, intermediate, lateral rostral, lateral caudal, caudal, and caudal limiting) were characterized for , , and . Our data indicated no influence of sex, or Braak and Braak staging on , , or . The volume and pial surface area for mean whole entorhinal cortex were 1131 ± 55.72 mm and 429 ± 22.6 mm (mean ± SEM), respectively. The subfield volume percentages relative to the entire entorhinal cortex were olfactory: 18.73 ± 1.82%, rostral: 14.06 ± 0.63%, lateral rostral: 14.81 ± 1.22%, medial intermediate: 6.72 ± 0.72%, intermediate: 23.36 ± 1.85%, lateral caudal: 5.42 ± 0.33%, caudal: 10.99 ± 1.02%, and caudal limiting: 5.91 ± 0.40% (all mean ± SEM). Olfactory and intermediate subfield revealed the most extensive intra-individual variability (cross-subject variance) in and This study provides validated measures. It maps individuality and demonstrates human variability in the entorhinal cortex, providing a baseline for approaches in individualized medicine. Taken together, this study serves as a ground-truth validation study for future comparisons and treatments.
神经影像学研究通常将海马体体积作为阿尔茨海默病严重程度的一项指标,但海马体的变化在疾病进程中出现得太晚,以至于潜在疗法难以发挥作用。内嗅皮质是最早受到阿尔茨海默病影响的皮质区域之一;其神经元特别容易受到神经原纤维缠结的影响。内嗅皮质萎缩也与从非临床阿尔茨海默病向临床阿尔茨海默病的转变有关。在神经影像学中,人类内嗅皮质目前大多被整体考虑,或被分为内侧和外侧区域。细胞构筑学差异为亚区域划分提供了机会。我们在阿尔茨海默病进展的关键时间点,在亚区域特异性水平上对内嗅皮质进行了研究。虽然磁共振成像(MRI)允许进行多维度定量测量,但只有组织学能提供足够的精度来确定亚区域边界——这是对内嗅皮质进行定量测量的先决条件。本研究使用组织学数据来验证超高分辨率7特斯拉MRI,并在总共10例临床前阿尔茨海默病和正常对照病例中创建内嗅皮质亚区域划分。使用MRI,确定了8个内嗅皮质亚区域(嗅觉、嘴侧部、内侧中间部、中间部、外侧嘴侧部、外侧尾侧部、尾侧部和尾侧界限部)的[具体参数未提及]、[具体参数未提及]和[具体参数未提及]。我们的数据表明,性别、Braak分期对[具体参数未提及]、[具体参数未提及]或[具体参数未提及]没有影响。整个内嗅皮质的平均体积和软脑膜表面积分别为1131±55.72立方毫米和429±22.6平方毫米(平均值±标准误)。相对于整个内嗅皮质,各亚区域的体积百分比分别为:嗅觉部:18.73±1.82%,嘴侧部:14.06±0.63%,外侧嘴侧部:14.81±1.22%,内侧中间部:6.72±0.72%,中间部:23.36±1.85%,外侧尾侧部:5.42±0.33%,尾侧部:10.99±1.02%,尾侧界限部:5.91±0.40%(均为平均值±标准误)。嗅觉和中间亚区域在[具体参数未提及]和[具体参数未提及]方面表现出个体内最大的变异性(个体间差异)。本研究提供了经过验证的测量方法。它描绘了个体差异,并展示了内嗅皮质的个体变异性,为个性化医疗方法提供了基线。综上所述,本研究为未来的[具体未提及]比较和治疗提供了一个基准验证研究。