Liew Bernard X W, Valera-Calero Juan Antonio, Varol Umut, Nijs Jo, Arendt-Nielsen Lars, Plaza-Manzano Gustavo, Fernández-de-Las-Peñas César
School of Sport, Rehabilitation and Exercise Sciences, University of Essex, Colchester CO4 3SQ, UK.
Department of Physiotherapy, Faculty of Health, Universidad Camilo José Cela, Villanueva de la Cañada, 28692 Madrid, Spain.
Biomedicines. 2022 May 20;10(5):1188. doi: 10.3390/biomedicines10051188.
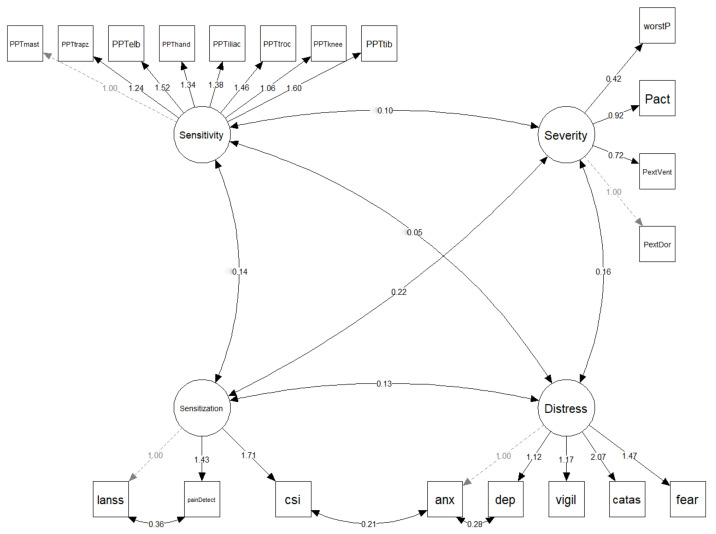
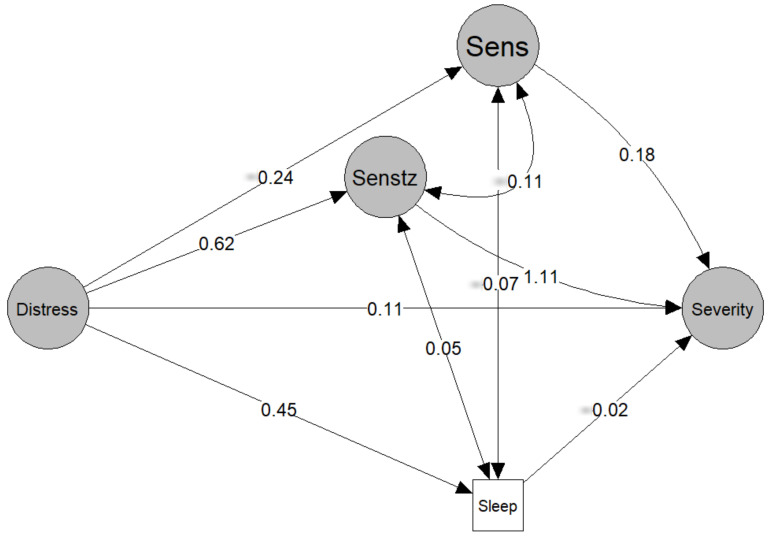
We aimed to explore a path model identified using a structural equation model (SEM) which best explains the multivariate contributions of sensitization, sensitivity, and emotional variables to clinical severity in women with FMS. Pain features, the Central Sensitization Inventory (CSI), painDETECT, S-LANSS, the Hospital Anxiety and Depression Scale (HADS), the Pittsburgh Sleep Quality Index (PSQI), the Pain Catastrophizing Scale (PCS), the Pain Vigilance and Awareness Questionnaire (PVAQ), the 11-item Tampa Scale for Kinesiophobia (TSK-11), and pressure pain thresholds (PPTs) were collected from 113 women with FMS. Four latent variables were created: severity (clinical pain features), sensitivity (PPTs), sensitization (S-LANSS, CSI, painDETECT), and distress (HADS-A, HADS-D, PCS, PVAQ, TSK-11). Data fit for the measurement model were considered excellent (RMSEA = 0.043, CFI = 0.966, SRMR = 0.067, and NNFI = 0.960). Distress had a significant relationship with the mediators of sleep (β = 0.452, p = 0.031) and sensitization (β = 0.618, p = 0.001). The only mediator with a significant effect (β = 1.113, p < 0.001) on severity was sensitization. A significant indirect effect of sensitization (β = 0.687, p = 0.001) that explained the relationship between distress and severity was also identified. The proposed model suggests that distress and sensitization, together with poor sleep, have a complex mediating effect on severity in women with FMS. The identified path model can be leveraged in clinical trials investigating treatment approaches for FMS.
我们旨在探索一种使用结构方程模型(SEM)确定的路径模型,该模型能最好地解释致敏、敏感性和情绪变量对纤维肌痛综合征(FMS)女性患者临床严重程度的多变量贡献。我们收集了113名FMS女性患者的疼痛特征、中枢致敏量表(CSI)、疼痛DETECT问卷、简化版神经病理性疼痛症状评估量表(S-LANSS)、医院焦虑抑郁量表(HADS)、匹兹堡睡眠质量指数(PSQI)、疼痛灾难化量表(PCS)、疼痛警觉与意识问卷(PVAQ)、11项坦帕运动恐惧量表(TSK-11)以及压痛阈值(PPTs)。创建了四个潜在变量:严重程度(临床疼痛特征)、敏感性(PPTs)、致敏(S-LANSS、CSI、疼痛DETECT)和痛苦(HADS-A、HADS-D、PCS、PVAQ、TSK-11)。测量模型的数据拟合被认为非常出色(RMSEA = 0.043,CFI = 0.966,SRMR = 0.067,NNFI = 0.960)。痛苦与睡眠介导因素(β = 0.452,p = 0.031)和致敏(β = 0.618,p = 0.001)存在显著关系。对严重程度有显著影响(β = 1.113,p < 0.001)的唯一介导因素是致敏。还确定了致敏的显著间接效应(β = 0.687,p = 0.001),该效应解释了痛苦与严重程度之间的关系。所提出的模型表明,痛苦、致敏以及睡眠不佳对FMS女性患者的严重程度具有复杂的介导作用。所确定的路径模型可用于调查FMS治疗方法的临床试验。