Department of Neurology, University of Goettingen Medical School, 37075 Goettingen, Germany.
Department of Neurology, University Hospital Giessen, 35394 Giessen, Germany.
Int J Mol Sci. 2022 May 11;23(10):5381. doi: 10.3390/ijms23105381.
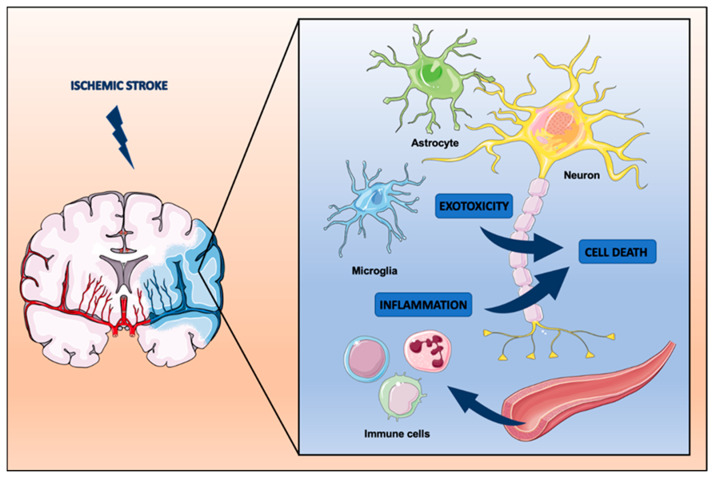
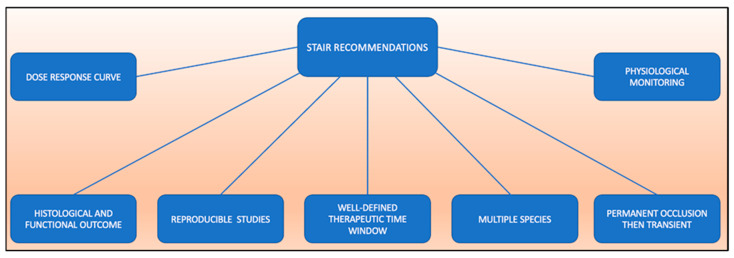
Despite tremendous progress in modern-day stroke therapy, ischemic stroke remains a disease associated with a high socioeconomic burden in industrialized countries. In light of demographic change, these health care costs are expected to increase even further. The current causal therapeutic treatment paradigms focus on successful thrombolysis or thrombectomy, but only a fraction of patients qualify for these recanalization therapies because of therapeutic time window restrictions or contraindications. Hence, adjuvant therapeutic concepts such as neuroprotection are urgently needed. A bench-to-bedside transfer of neuroprotective approaches under stroke conditions, however, has not been established after more than twenty years of research, albeit a great many data have demonstrated several neuroprotective drugs to be effective in preclinical stroke settings. Prominent examples of substances supported by extensive preclinical evidence but which failed clinical trials are tirilazad and disodium 2,4-sulphophenyl-N-tert-butylnitrone (NXY-059). The NXY-059 trial, for instance, was retrospectively shown to have a seriously weak study design, a trial of insufficient quality and a poor statistical analysis, although it initially met the recommendations of the STAIR committee. In light of currently ongoing novel neuroprotective stroke trials, such as ESCAPE-NA, and to avoid the mistakes made in the past, an improvement in study quality in the field of stroke neuroprotection is urgently needed. In the present review, animal models closely reflecting the "typical" stroke patient, occlusion techniques and the appropriate choice of time windows are discussed. In this context, the STAIR recommendations could provide a useful orientation. Taking all of this into account, a new dawn for neuroprotection might be possible.
尽管现代中风治疗取得了巨大进展,但在工业化国家,缺血性中风仍然是一种与高社会经济负担相关的疾病。鉴于人口结构的变化,这些医疗保健费用预计将进一步增加。目前的因果治疗模式侧重于成功的溶栓或血栓切除术,但由于治疗时间窗限制或禁忌症,只有一部分患者有资格接受这些再通治疗。因此,迫切需要辅助治疗概念,如神经保护。尽管经过二十多年的研究,在中风情况下,从实验室到临床的神经保护方法的转化尚未建立,尽管有大量数据表明几种神经保护药物在临床前中风环境中是有效的。有大量临床前证据支持但临床试验失败的突出例子是替拉扎特和二钠 2,4-磺苯基-N-叔丁基硝酮(NXY-059)。例如,尽管 NXY-059 试验最初符合 STAIR 委员会的建议,但从回顾性研究中可以看出,该试验的研究设计严重薄弱,试验质量不高,统计分析也不佳。鉴于目前正在进行的新型神经保护中风试验,如 ESCAPE-NA,为避免过去的错误,迫切需要提高中风神经保护领域的研究质量。在本综述中,讨论了更紧密地反映“典型”中风患者的动物模型、闭塞技术和适当的时间窗选择。在这方面,STIR 建议可以提供有用的指导。考虑到所有这些因素,神经保护可能会迎来新的曙光。