Wang Qingqing, Zhang Jie, Xu Liu, Li Xiaohuan, Lu Yifan, Chen Songhai, Jin Qianhui
Department of General Surgery, The First Hospital of Jiaxing (The First Affiliated Hospital of Jiaxing University), Jiaxing, Zhejiang 314001, PR China.
Department of General Surgery, The First Hospital of Jiaxing (The First Affiliated Hospital of Jiaxing University), Jiaxing, Zhejiang 314001, PR China.
Int J Surg Case Rep. 2022 Jun;95:107176. doi: 10.1016/j.ijscr.2022.107176. Epub 2022 May 10.
Primary hepatic neuroendocrine tumors (PHNETs) are extremely rare, and the clinical symptoms, test results, and imaging characteristics are nonspecific in most patients; thus, it is difficult to differentiate from other liver masses before surgery. Histopathology and immunohistochemistry are the main basis for the diagnosis. PHNETs and colon tumors co-occur in a patient and are non-homologous, as reported in the English-language literature for the first time.
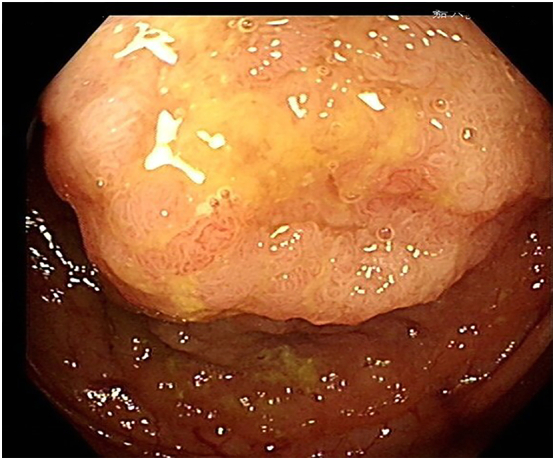
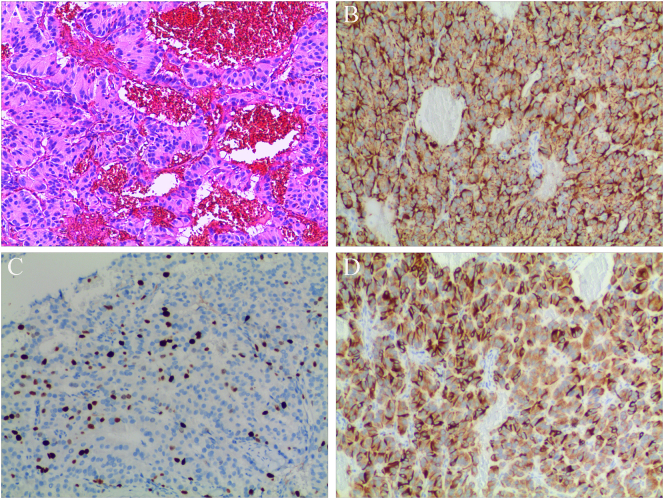
We present a case of a 60-year-old woman with right hepatic lobe mass accidentally discovered on abdominal ultrasonography during a routine examination. Preoperative liver contrast-enhanced computed tomography suggested hepatocellular carcinoma; then, surgery were performed. Pathological results revealed a Grade 2 neuroendocrine tumor of the liver. In search of the primary tumor, upper and lower endoscopy of the GI tract was performed and revealed a mass in the ascending colon. Ascending colon cancer was considered; then, laparoscopic right hemicolectomy was performed. Pathological results suggested tubular villous adenoma of the ascending colon. The final diagnosis was not colon cancer with liver metastases but was PHNETs with colon adenoma.
PHNETs are rare cancers that are difficult to diagnose, requiring not only differentiation from other liver masses but also exclusion of metastases from extrahepatic sources. The pathological results play an important in making an accurate diagnosis.
Pathology, postoperative follow-up, and comprehensive imaging examinations are powerful tools in the diagnosis of PHNETs. Currently, surgery is the best treatment to achieve a potential cure and prolong the patient's survival.
原发性肝神经内分泌肿瘤(PHNETs)极为罕见,大多数患者的临床症状、检查结果及影像学特征均无特异性,因此术前难以与其他肝脏肿块相鉴别。组织病理学和免疫组织化学是诊断的主要依据。据英文文献首次报道,一名患者同时出现PHNETs和结肠肿瘤,且二者不同源。
我们报告一例60岁女性患者,在常规检查中腹部超声偶然发现右肝叶肿块。术前肝脏增强CT提示肝细胞癌,随后进行了手术。病理结果显示为2级肝神经内分泌肿瘤。为寻找原发肿瘤,对胃肠道进行了上下消化道内镜检查,发现升结肠有一肿块。考虑为升结肠癌,随后进行了腹腔镜右半结肠切除术。病理结果提示为升结肠管状绒毛状腺瘤。最终诊断并非结肠癌肝转移,而是PHNETs合并结肠腺瘤。
PHNETs是罕见癌症,诊断困难,不仅需要与其他肝脏肿块相鉴别,还需排除肝外来源的转移。病理结果对准确诊断至关重要。
病理学、术后随访及综合影像学检查是诊断PHNETs的有力工具。目前,手术是实现潜在治愈并延长患者生存期的最佳治疗方法。