Division of Rheumatology and Research, Diakonhjemmet Hospital, Box 23 Vinderen, 0319, Oslo, Norway.
Division of Rheumatology, Inflammation, and Immunity, Department of Medicine, Brigham and Women's Hospital/Harvard Medical School, Boston, USA.
BMC Med Res Methodol. 2022 May 28;22(1):152. doi: 10.1186/s12874-022-01639-0.
Observational data are increasingly being used to conduct external comparisons to clinical trials. In this study, we empirically examined whether different methodological approaches to longitudinal missing data affected study conclusions in this setting.
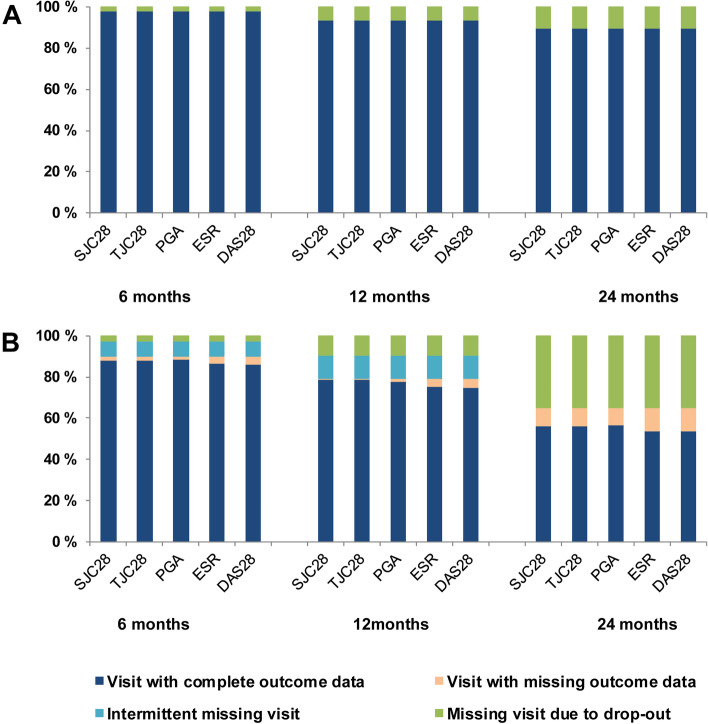
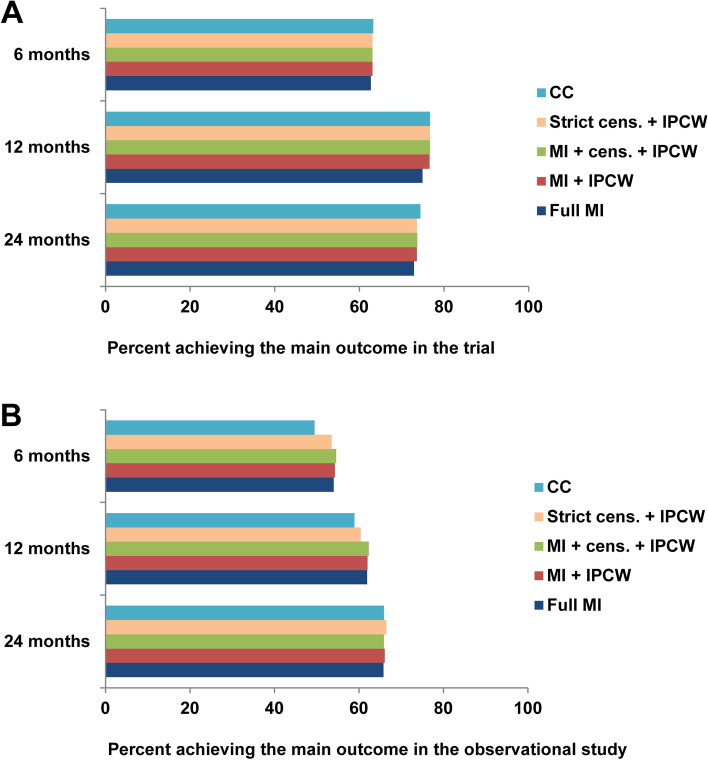
We used data from one clinical trial and one prospective observational study, both Norwegian multicenter studies including patients with recently diagnosed rheumatoid arthritis and implementing similar treatment strategies, but with different stringency. A binary disease remission status was defined at 6, 12, and 24 months in both studies. After identifying patterns of longitudinal missing outcome data, we evaluated the following five approaches to handle missingness: analyses of patients with complete follow-up data, multiple imputation (MI), inverse probability of censoring weighting (IPCW), and two combinations of MI and IPCW.
We found a complex non-monotone missing data pattern in the observational study (N = 328), while missing data in the trial (N = 188) was monotone due to drop-out. In the observational study, only 39.0% of patients had complete outcome data, compared to 89.9% in the trial. All approaches to missing data indicated favorable outcomes of the treatment strategy in the trial and resulted in similar study conclusions. Variations in results across approaches were mainly due to variations in estimated outcomes for the observational data.
Five different approaches to handle longitudinal missing data resulted in similar conclusions in our example. However, the extent and complexity of missing observational data affected estimated comparative outcomes across approaches, highlighting the need for careful consideration of methods to account for missingness in this setting. Based on this empirical examination, we recommend using a prespecified advanced missing data approach to account for longitudinal missing data, and to conduct alternative approaches in sensitivity analyses.
观察性数据越来越多地被用于与临床试验进行外部比较。在这项研究中,我们实证检验了在这种情况下,不同的纵向缺失数据方法是否会影响研究结论。
我们使用了一项临床试验和一项前瞻性观察性研究的数据,这两项研究均为挪威多中心研究,纳入了近期诊断为类风湿关节炎的患者,实施了类似的治疗策略,但严格程度不同。在两项研究中,均在 6、12 和 24 个月时定义疾病缓解的二元状态。在确定纵向缺失结局数据的模式后,我们评估了以下五种处理缺失数据的方法:对具有完整随访数据的患者进行分析、多重插补(MI)、逆概率 censoring 加权(IPCW),以及 MI 和 IPCW 的两种组合。
我们发现观察性研究(N=328)中的缺失数据模式复杂且非单调,而试验(N=188)中的缺失数据由于脱落呈单调趋势。在观察性研究中,只有 39.0%的患者具有完整的结局数据,而在试验中这一比例为 89.9%。所有处理缺失数据的方法均表明试验中治疗策略的结局良好,并得出了相似的研究结论。不同方法的结果差异主要是由于观察性数据的估计结局不同。
在我们的例子中,五种不同的方法处理纵向缺失数据得出了相似的结论。然而,观察性缺失数据的程度和复杂性会影响不同方法的估计比较结局,这突出了在这种情况下需要仔细考虑方法来处理缺失数据的必要性。基于这项实证检验,我们建议使用预先指定的高级缺失数据方法来处理纵向缺失数据,并在敏感性分析中进行替代方法。