Raphael Ari, Onn Amir, Holtzman Liran, Dudnik Julia, Urban Damien, Kian Waleed, Cohen Aharon Y, Moskovitz Mor, Zer Alona, Bar Jair, Rabinovich Natalie Maimon, Grynberg Shirly, Oedegaard Cecilie, Agbarya Abed, Peled Nir, Shochat Tzippy, Dudnik Elizabeth
Department of Oncology, Tel-Aviv Sourasky Medical Center, Tel-Aviv, Israel.
Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel.
Front Oncol. 2022 May 13;12:874712. doi: 10.3389/fonc.2022.874712. eCollection 2022.
The use of CGP in guiding treatment decisions in aNSCLC with acquired resistance to ALK TKIs is questionable.
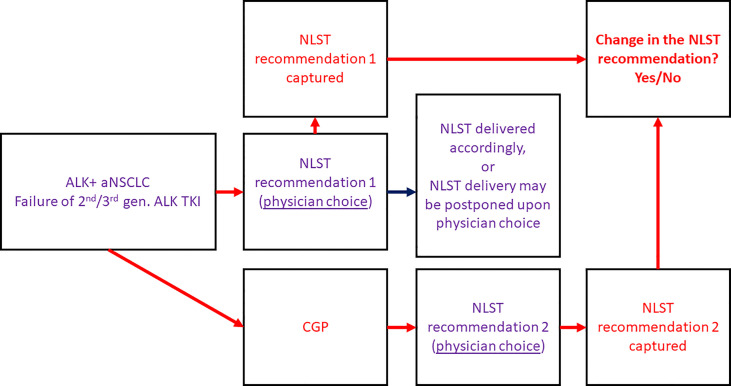
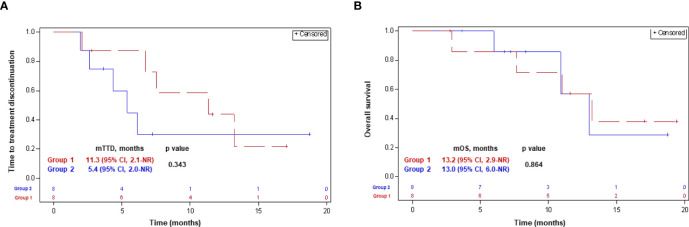
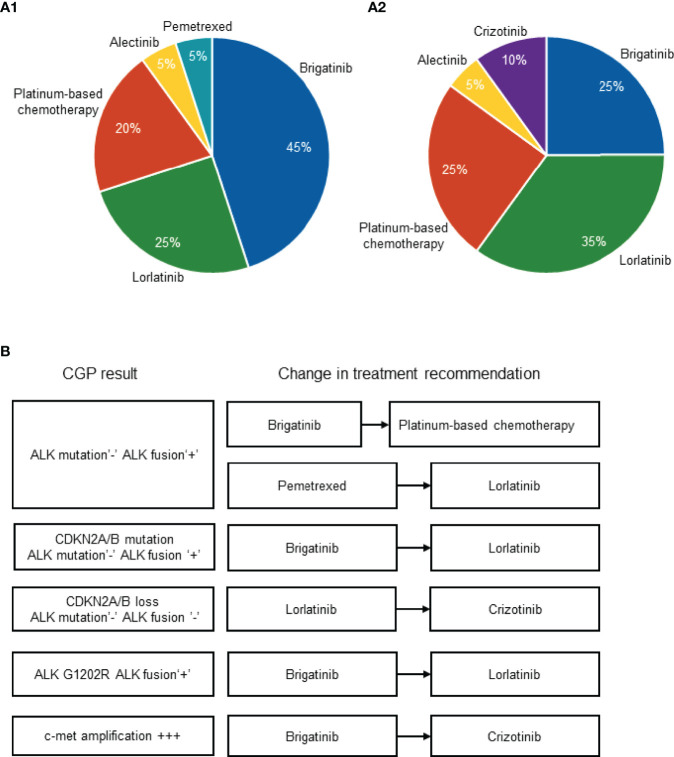
We prospectively assessed the impact of CGP on the decision-making process in ALK-rearranged aNSCLC patients following progression on 2/3-generation ALK TKIs. Physician's choice of the most recommended next-line systemic treatment (NLST) was captured before and after receival of CGP results; the percentage of cases in which the NLST recommendation has changed was assessed along with the CGP turnaround time (TAT). Patients were divided into groups: patients in whom the NLST was initiated after (group 1) and before (group 2) receival of the CGP results. Time-to-treatment discontinuation (TTD) and overall survival (OS) with NLST were compared between the groups.
In 20 eligible patients (median [m]age 63 years [range, 40-89], females 75%, adenocarcinoma 100%, failure of alectinib 90%, FoundationOne Liquid CDx 80%), CGP has altered NLST recommendation in 30% of cases. CGP findings were as follows: ALK mutations 30% (l1171X 10%, G1202R, L1196M, G1269A, G1202R+l1171N+E1210K 5% each), CDKN2A/B mutation/loss 10%, c-met amplification 5%. CGP mTAT was 2.9 weeks [IQR, 2.4-4.4]. mTTD was 11.3 months (95% CI, 2.1-not reached [NR]) and 5.4 months (95% CI, 2.0-NR) in groups 1 and 2, respectively (p-0.34). mOS was 13.2 months (95% CI, 2.9-NR) and 13.0 months (95% CI, 6.0-NR) in groups 1 and 2, respectively (p-0.86).
CGP has a significant impact on the decision-making process in ALK-rearranged aNSCLC following progression on 2/3-generation ALK TKIs.
在对ALK酪氨酸激酶抑制剂(TKIs)产生获得性耐药的晚期非小细胞肺癌(aNSCLC)中,使用循环肿瘤基因图谱(CGP)指导治疗决策存在疑问。
我们前瞻性评估了CGP对接受2/3代ALK TKIs治疗后病情进展的ALK重排aNSCLC患者决策过程的影响。在获得CGP结果之前和之后,记录医生选择的最推荐的二线全身治疗(NLST);评估NLST推荐发生改变的病例百分比以及CGP周转时间(TAT)。将患者分为两组:在获得CGP结果之后(第1组)和之前(第2组)开始NLST的患者。比较两组之间NLST的治疗中断时间(TTD)和总生存期(OS)。
在20例符合条件的患者中(中位年龄63岁[范围40 - 89岁],女性占75%,腺癌占100%,阿来替尼治疗失败的占90%,FoundationOne Liquid CDx检测的占80%),CGP在30%的病例中改变了NLST推荐。CGP检测结果如下:ALK突变占30%(L1171X占10%,G1202R、L1196M、G1269A、G1202R + L1171N + E1210K各占5%),CDKN2A/B突变/缺失占10%,c-met扩增占5%。CGP的中位TAT为2.9周[四分位间距,2.4 - 4.4]。第1组和第2组的中位TTD分别为11.3个月(95%置信区间,2.1 - 未达到[NR])和5.4个月(95%置信区间,2.0 - NR)(p = 0.34)。第1组和第2组的中位OS分别为13.2个月(95%置信区间,2.9 - NR)和13.0个月(95%置信区间,6.0 - NR)(p = 0.86)。
在接受2/3代ALK TKIs治疗后病情进展的ALK重排aNSCLC中,CGP对决策过程有显著影响。