Filetti Marco, Lombardi Pasquale, Falcone Rosa, Giusti Raffaele, Giannarelli Diana, Carcagnì Antonella, Altamura Valeria, Scambia Giovanni, Daniele Gennaro
Phase 1 Unit, Fondazione Policlinico Universitario A. Gemelli IRCCS, 00168 Rome, Italy.
Department of Experimental Medicine, Sapienza University of Rome, 00168 Rome, Italy.
Explor Target Antitumor Ther. 2023;4(6):1136-1144. doi: 10.37349/etat.2023.00187. Epub 2023 Dec 1.
This article is based on our previous research, which was presented as a post at the Congress Aiom 2022 Congress and published in as Conference Abstract (. 2022;108:1-194. doi: 10.1177/03008916221114500). In this paper, a comprehensive presentation of all the achieved results is provided. Several tyrosine kinase inhibitors (TKIs) have been investigated to treat patients with anaplastic lymphoma kinase (ALK)-positive non-small cell lung cancer (NSCLC). However, direct comparisons between these TKIs are lacking, with many only being compared to crizotinib. To address this gap, a network meta-analysis was conducted to compare the efficacy and safety of various first-line systemic therapies for ALK-positive NSCLC.
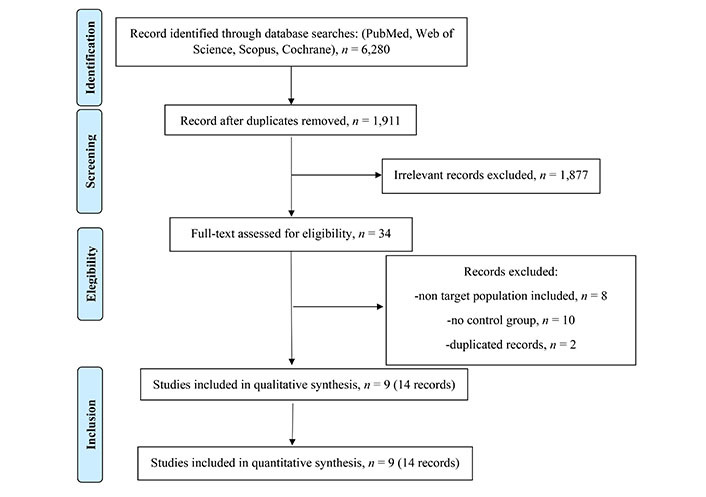
A thorough search of PubMed, Embase, and Cochrane Library was performed to identify randomized controlled trials (RCTs) published between January 01, 2000 and April 01, 2022, and included trials that investigated upfront treatments for this molecular subgroup and reported overall survival (OS), progression-free survival (PFS), objective response rate (ORR), and adverse events (AEs) of grade 3 or higher (grade ≥ 3 AEs).
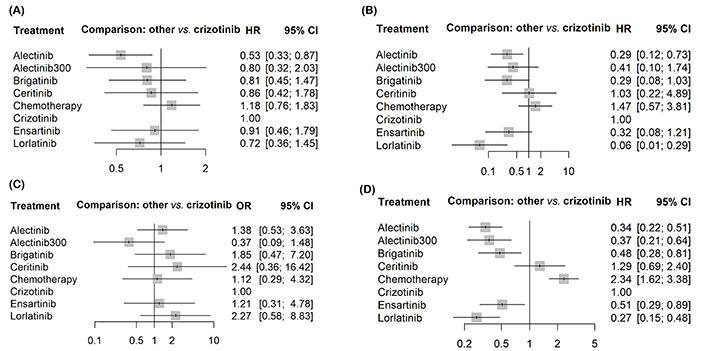
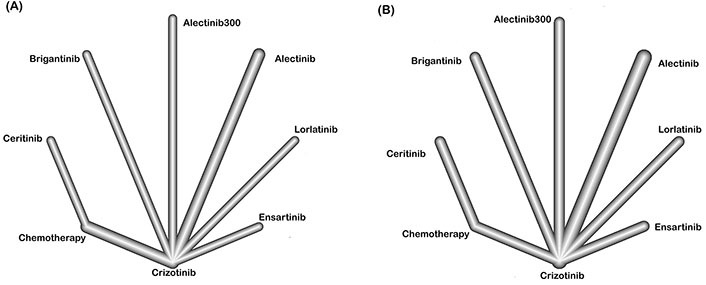
The analysis included 9 RCTs with 2,443 patients receiving eight different treatments: alectinib (at two different dosages), brigatinib, ceritinib, crizotinib, ensartinib, lorlatinib, and chemotherapy. Second and third-generation TKIs significantly prolonged PFS compared to crizotinib, with lorlatinib having the highest probability of yielding the most favorable PFS, followed by alectinib (300 mg or 600 mg). However, only alectinib has been shown to significantly prolong OS compared to crizotinib to date. Lorlatinib appears superior in reducing the risk of central nervous system (CNS) progression, followed by alectinib 600 mg. Ceritinib had the highest rate of AEs, followed by lorlatinib and brigatinib.
Based on the network meta-analysis, alectinib and lorlatinib emerged as the most promising upfront treatment options. These treatments provide prolonged disease control while maintaining an acceptable safety profile.
本文基于我们之前的研究,该研究在2022年艾奥姆大会上作为一篇海报展示,并以会议摘要形式发表(. 2022;108:1 - 194. doi: 10.1177/03008916221114500)。本文全面展示了所有已取得的成果。已经研究了几种酪氨酸激酶抑制剂(TKIs)用于治疗间变性淋巴瘤激酶(ALK)阳性非小细胞肺癌(NSCLC)患者。然而,这些TKIs之间缺乏直接比较,许多仅与克唑替尼进行了比较。为填补这一空白,进行了一项网状Meta分析,以比较ALK阳性NSCLC各种一线全身治疗的疗效和安全性。
对PubMed、Embase和Cochrane图书馆进行全面检索,以识别2000年1月1日至2022年4月1日期间发表的随机对照试验(RCTs),纳入研究该分子亚组一线治疗并报告总生存期(OS)、无进展生存期(PFS)、客观缓解率(ORR)以及3级或更高等级不良事件(AEs)(≥3级AEs)的试验。
该分析纳入了9项RCTs,共2443例患者接受了8种不同治疗:阿来替尼(两种不同剂量)、布加替尼、塞瑞替尼、克唑替尼、恩沙替尼、劳拉替尼和化疗。与克唑替尼相比,第二代和第三代TKIs显著延长了PFS,其中劳拉替尼产生最有利PFS的概率最高,其次是阿来替尼(300mg或600mg)。然而,迄今为止,只有阿来替尼被证明与克唑替尼相比能显著延长OS。劳拉替尼在降低中枢神经系统(CNS)进展风险方面似乎更具优势,其次是阿来替尼600mg。塞瑞替尼的AEs发生率最高,其次是劳拉替尼和布加替尼。
基于网状Meta分析,阿来替尼和劳拉替尼成为最有前景的一线治疗选择。这些治疗在维持可接受安全性的同时提供了更长时间的疾病控制。