Research Laboratory LR12SP18, Monastir University, Monastir, Tunisia.
Emergency Department and Laboratory Research (LR12SP18), Fattouma Bourguiba University Hospital, Monastir, Tunisia.
Ther Adv Respir Dis. 2022 Jan-Dec;16:17534666221099729. doi: 10.1177/17534666221099729.
Duration of antibiotic treatment in acute exacerbation of COPD (AECOPD) is most commonly based on expert opinion. Typical administration periods range from 5 to 7 days. A 2-day course with levofloxacin was not previously assessed. We performed a randomized clinical trial to evaluate the efficacy of 2-day 7-day treatment with levofloxacin in patients with AECOPD.
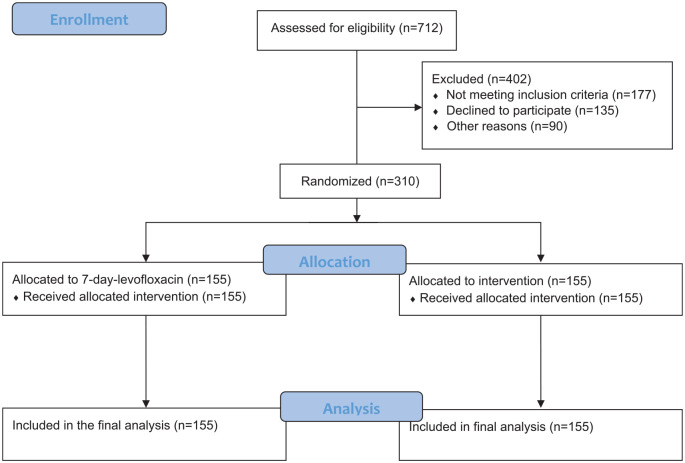
Patients with AECOPD were randomized to receive levofloxacin for 2 days and 5 days placebo ( = 155) or levofloxacin for 7 days ( = 155). All patients received a common dose of intravenous prednisone daily for 5 days. The primary outcome measure was cure rate, and secondary outcomes included need for additional antibiotics, ICU admission rate, re-exacerbation rate, death rate, and exacerbation-free interval (EFI) within 1-year follow-up. The study protocol has been prepared in accordance with the revised Helsinki Declaration for Biomedical Research Involving Human Subjects and Guidelines for Good Clinical Practice. The study was approved by ethics committees of all participating centers prior to implementation (Monastir and Sousse Universities).
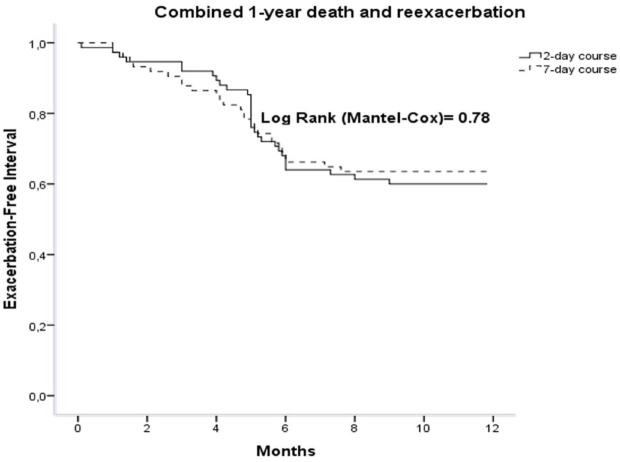
310 patients were randomized to receive 2-day course of levofloxacin ( = 155) or 7-day course ( = 155). Cure rate was 79.3% ( = 123) and 74.2% ( = 115), respectively, in 2-day and 7-day groups [OR 1.3; 95% CI 0.78-2.2 ( = 0.28)]. Need for additional antibiotics rate was 3.2% and 1.9% in the 2-day group and 7-day group, respectively; ( = 0.43). ICU admission rate was not significantly different between both groups. One-year re-exacerbation rate was 34.8% ( = 54) in 2-day group 29% ( = 45) in 7-day group ( = 0.19); the EFI was 121 days (interquartile range, 99-149) 110 days (interquartile range, 89-132) in 2-day and 7-day treatment groups, respectively; ( = 0.73). One-year death rate was not significantly different between the 2 groups, 5.2% 7.1% in the 2-day group and 7-day group, respectively; ( = 0.26). No difference in adverse effects was detected.
Levofloxacin once daily for 2 days is not inferior to 7 days with respect to cure rate, need for additional antibiotics and hospital readmission in AECOPD. Our findings would improve patient compliance and reduce the incidence of bacterial resistance and adverse effects.
慢性阻塞性肺疾病急性加重(AECOPD)的抗生素治疗时间通常基于专家意见。典型的治疗期为 5 至 7 天。左氧氟沙星的 2 天疗程以前未进行评估。我们进行了一项随机临床试验,以评估左氧氟沙星在 AECOPD 患者中 2 天和 7 天疗程的疗效。
将 AECOPD 患者随机分为左氧氟沙星 2 天和 5 天安慰剂组( = 155)或左氧氟沙星 7 天组( = 155)。所有患者均接受每日静脉注射泼尼松龙 5 天的常规剂量。主要疗效指标为治愈率,次要疗效指标包括需要额外使用抗生素、入住 ICU 率、再加重率、死亡率和 1 年随访期内的无加重间隔(EFI)。研究方案符合涉及人类受试者的生物医学研究修订后的赫尔辛基宣言和良好临床实践指南。在实施之前,所有参与中心的伦理委员会均批准了该研究(突尼斯莫纳斯提尔大学和苏塞大学)。
310 名患者被随机分配接受 2 天左氧氟沙星疗程( = 155)或 7 天疗程( = 155)。2 天组和 7 天组的治愈率分别为 79.3%( = 123)和 74.2%( = 115)[比值比 1.3;95%置信区间 0.78-2.2( = 0.28)]。2 天组和 7 天组分别有 3.2%和 1.9%的患者需要额外使用抗生素( = 0.43)。两组 ICU 入院率无显著差异。2 天组和 7 天组的 1 年再加重率分别为 34.8%( = 54)和 29%( = 45)( = 0.19);2 天组和 7 天组的 EFI 分别为 121 天(四分位距,99-149)和 110 天(四分位距,89-132)( = 0.73)。两组 1 年死亡率无显著差异,分别为 5.2%( = 123)和 7.1%( = 115)( = 0.26)。未发现不良反应有差异。
左氧氟沙星每日 1 次,使用 2 天与 7 天相比,在 AECOPD 患者的治愈率、需要额外使用抗生素和住院再入院方面没有差异。我们的发现将提高患者的依从性,并降低细菌耐药性和不良反应的发生率。