Division of Headache and Facial Pain, Department of Neurology and Neurological Sciences, Stanford University School of Medicine, Stanford, California, USA.
Neurology, University of California, Los Angeles, California, USA.
Headache. 2022 Jul;62(7):870-882. doi: 10.1111/head.14324. Epub 2022 Jun 3.
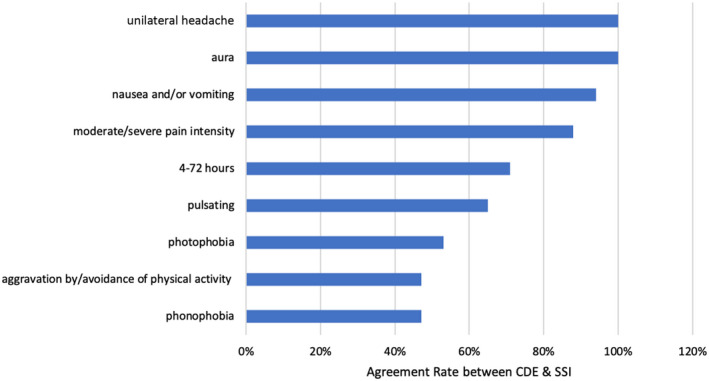
This study assesses the concordance in migraine diagnosis between an online, self-administered, Computer-based, Diagnostic Engine (CDE) and semi-structured interview (SSI) by a headache specialist, both using International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria.
Delay in accurate diagnosis is a major barrier to headache care. Accurate computer-based algorithms may help reduce the need for SSI-based encounters to arrive at correct ICHD-3 diagnosis.
Between March 2018 and August 2019, adult participants were recruited from three academic headache centers and the community via advertising to our cross-sectional study. Participants completed two evaluations: phone interview conducted by headache specialists using the SSI and a web-based expert questionnaire and analytics, CDE. Participants were randomly assigned to either the SSI followed by the web-based questionnaire or the web-based questionnaire followed by the SSI. Participants completed protocols a few minutes apart. The concordance in migraine/probable migraine (M/PM) diagnosis between SSI and CDE was measured using Cohen's kappa statistics. The diagnostic accuracy of CDE was assessed using the SSI as reference standard.
Of the 276 participants consented, 212 completed both SSI and CDE (study completion rate = 77%; median age = 32 years [interquartile range: 28-40], female:male ratio = 3:1). Concordance in M/PM diagnosis between SSI and CDE was: κ = 0.83 (95% confidence interval [CI]: 0.75-0.91). CDE diagnostic accuracy: sensitivity = 90.1% (118/131), 95% CI: 83.6%-94.6%; specificity = 95.8% (68/71), 95% CI: 88.1%-99.1%. Positive and negative predictive values = 97.0% (95% CI: 91.3%-99.0%) and 86.6% (95% CI: 79.3%-91.5%), respectively, using identified migraine prevalence of 60%. Assuming a general migraine population prevalence of 10%, positive and negative predictive values were 70.3% (95% CI: 43.9%-87.8%) and 98.9% (95% CI: 98.1%-99.3%), respectively.
The SSI and CDE have excellent concordance in diagnosing M/PM. Positive CDE helps rule in M/PM, through high specificity and positive likelihood ratio. A negative CDE helps rule out M/PM through high sensitivity and low negative likelihood ratio. CDE that mimics SSI logic is a valid tool for migraine diagnosis.
本研究通过使用国际头痛疾病分类第 3 版(ICHD-3)标准的在线、自我管理的基于计算机的诊断引擎(CDE)和头痛专家的半结构化访谈(SSI),评估偏头痛诊断在两者之间的一致性。
准确诊断的延迟是头痛护理的主要障碍。准确的基于计算机的算法可能有助于减少基于 SSI 的就诊次数,以得出正确的 ICHD-3 诊断。
2018 年 3 月至 2019 年 8 月,通过在我们的横断面研究中向三个学术头痛中心和社区发布广告,从三个学术头痛中心和社区招募成年参与者。参与者完成了两项评估:由头痛专家通过 SSI 进行的电话访谈和基于网络的专家问卷和分析,CDE。参与者被随机分配到 SSI 后进行基于网络的问卷或基于网络的问卷后进行 SSI。参与者在几分钟内完成方案。通过 Cohen's kappa 统计量测量 SSI 和 CDE 之间偏头痛/可能偏头痛(M/PM)诊断的一致性。使用 SSI 作为参考标准评估 CDE 的诊断准确性。
在 276 名同意的参与者中,有 212 名完成了 SSI 和 CDE(研究完成率为 77%;中位数年龄为 32 岁[四分位距:28-40],男女比例为 3:1)。SSI 和 CDE 之间 M/PM 诊断的一致性为:κ=0.83(95%置信区间[CI]:0.75-0.91)。CDE 的诊断准确性:敏感性为 90.1%(118/131),95%CI:83.6%-94.6%;特异性为 95.8%(68/71),95%CI:88.1%-99.1%。阳性和阴性预测值分别为 97.0%(95%CI:91.3%-99.0%)和 86.6%(95%CI:79.3%-91.5%),分别使用确定的偏头痛患病率为 60%。假设一般偏头痛人群患病率为 10%,阳性和阴性预测值分别为 70.3%(95%CI:43.9%-87.8%)和 98.9%(95%CI:98.1%-99.3%)。
SSI 和 CDE 在诊断 M/PM 方面具有极好的一致性。阳性 CDE 通过高特异性和阳性似然比有助于诊断 M/PM。阴性 CDE 通过高灵敏度和低阴性似然比有助于排除 M/PM。模仿 SSI 逻辑的 CDE 是偏头痛诊断的有效工具。