Millennium Health, San Diego, California.
Department of Biomedical Informatics, The Ohio State University, Columbus.
JAMA Netw Open. 2022 Jun 1;5(6):e2215425. doi: 10.1001/jamanetworkopen.2022.15425.
Drug overdose deaths in the US are currently the highest ever recorded; data collected from public health surveillance sources can help to identify emerging drug use patterns associated with overdose mortality rates, but the time lag in results often limits utility. Urine drug testing (UDT) is one potentially underused source that could augment surveillance efforts through timely data collection.
To evaluate the correlation between real-time UDT results from a proprietary national database and overdose mortality data from the National Vital Statistics System.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cross-sectional study included 500 000 urine specimens submitted for UDT by substance use disorder (SUD) treatment health care practices and collected between January 1, 2013, and December 31, 2020. Real-time UDT data were obtained from the Millennium Health proprietary national database, and overdose mortality data were obtained from the National Vital Statistics System of the Centers for Disease Control and Prevention (CDC WONDER). Specimens were analyzed for specific drugs in 5 categories (cocaine, heroin, methamphetamine, synthetic opioids, and other opioids) using liquid chromatography-tandem mass spectrometry. Participants were adults aged 18 years and older who provided urine specimens at SUD treatment practices.
Urine drug testing.
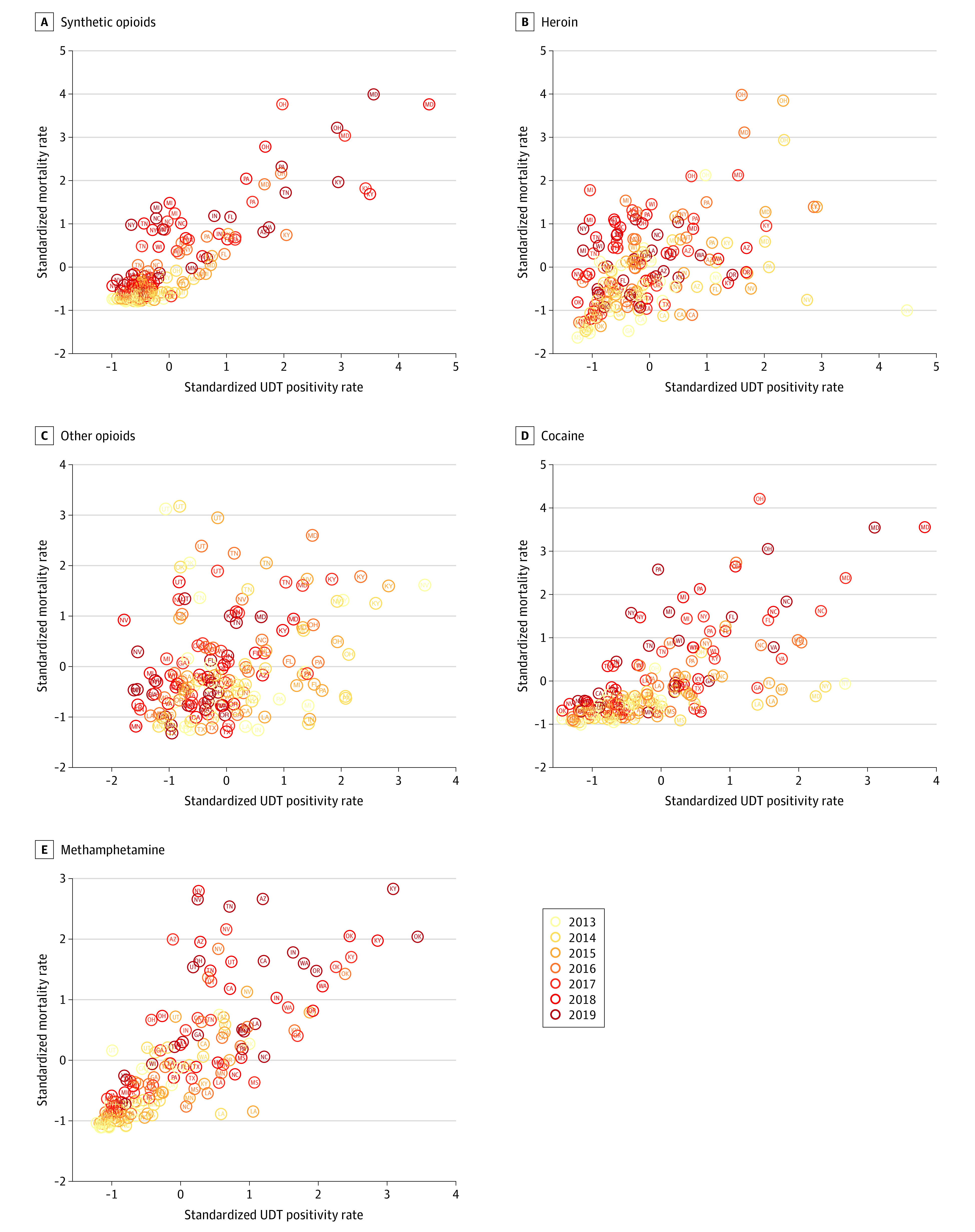
The primary outcome was the correlation between UDT positivity rates and overdose mortality rates at national, state, and county levels. Univariate and multivariate regression models were also used to evaluate the association between state- and county-level overdose mortality and standardized UDT positivity rates.
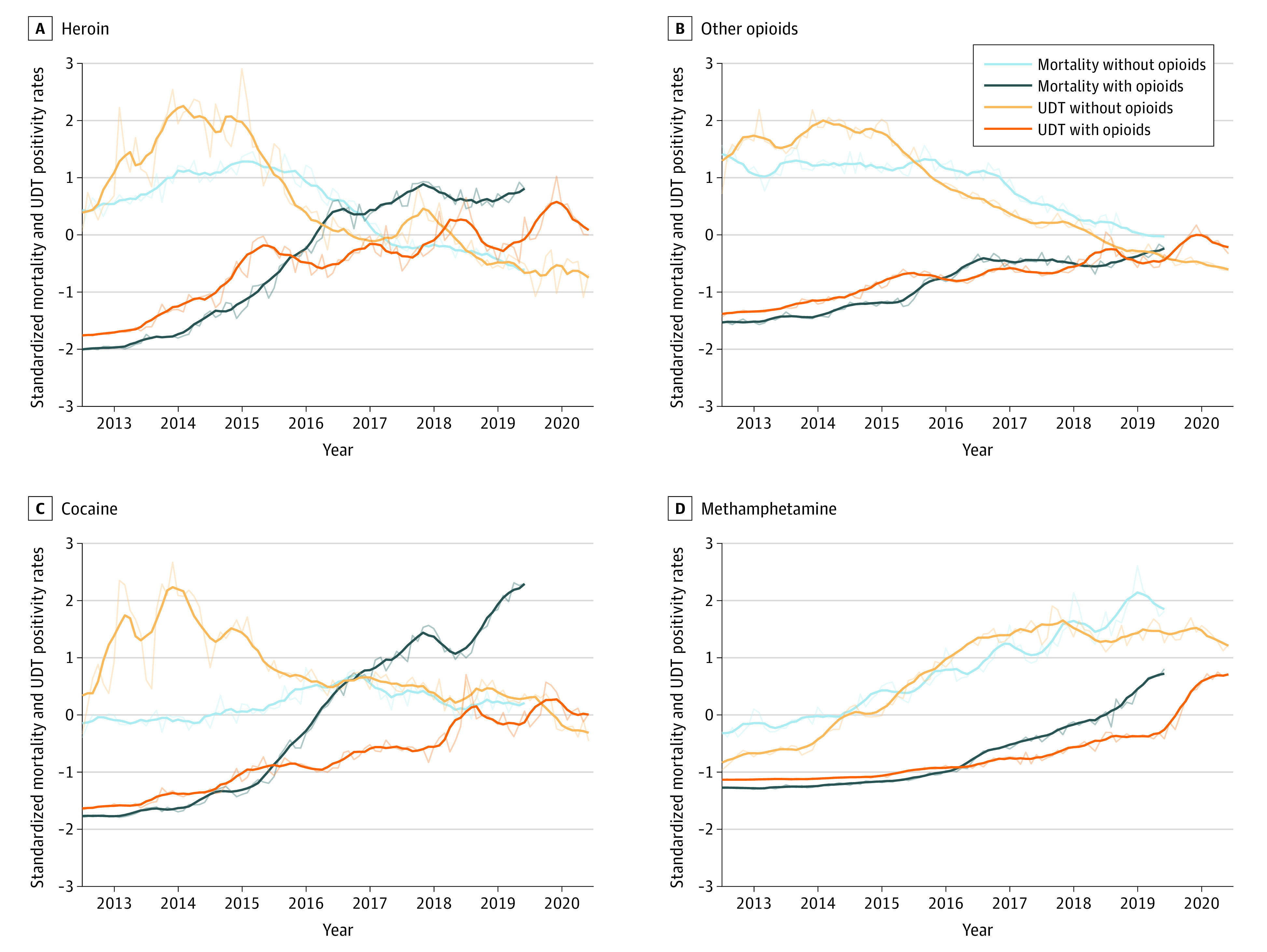
Among 500 000 unique patient specimens collected from SUD treatment practices between 2013 and 2020, 288 534 specimens (57.7%) were from men, and the median age of the study population was 34 years (IQR, 17-51 years). On a national level, synthetic opioids and methamphetamine were highly correlated with overdose mortality (Spearman ρ = 0.96 for both). When synthetic opioids were coinvolved, methamphetamine (ρ = 0.98), heroin (ρ = 0.78), cocaine (ρ = 0.94), and other opioids (ρ = 0.83) were also highly correlated with overdose mortality. In the absence of synthetic opioids, all drug categories were highly correlated (ρ = 0.75 for other opioids, 0.81 for heroin, and 0.88 for methamphetamine), with the exception of cocaine (ρ = -0.37). Synthetic opioids (ρ = 0.77) and methamphetamine (ρ = 0.80) had the strongest state-level correlations over time, whereas other opioids had the lowest correlation for both total positivity (ρ = 0.31) and positivity in the absence of synthetic opioids (ρ = 0.23). In Ohio, county-level correlation was strongest for synthetic opioids (ρ = 0.71), followed by heroin (ρ = 0.69) and methamphetamine (ρ = 0.67). At the state level, the multivariate incidence rate ratio (IRR) for synthetic opioids was 1.16 (95% CI, 1.14-1.19; P < .001), and at the county level, the IRR was 1.13 (95% CI, 1.09-1.17; P < .001), suggesting that for every 1-SD increase in the UDT positivity rate, there were 16.2% and 12.8% increases, respectively, in monthly overdose deaths. Both methamphetamine (11.7% increase per 1-SD increase in UDT positivity rate; IRR, 1.12; 95% CI, 1.09-1.14; P < .001) and cocaine (5.1% increase per 1-SD increase in UDT positivity rate; IRR, 1.05; 95% CI, 1.03-1.07; P < .001) also had significant positive associations with mortality rates, but the effect sizes were smaller than that of synthetic opioids (IRR, 1.16).
In this study, UDT results were highly correlated with mortality rates at national, state, and county levels. These findings suggest that real-time UDT surveillance can help to quickly identify changes in drug use patterns that might inform targeted harm reduction strategies designed to prevent overdose deaths.
美国的药物过量死亡人数目前处于历史最高水平;从公共卫生监测来源收集的数据可以帮助确定与过量死亡率相关的新的药物使用模式,但结果的时间滞后往往限制了其效用。尿液药物检测(UDT)是一种潜在的未充分利用的资源,可以通过及时的数据收集来增强监测工作。
评估来自专有国家数据库的实时 UDT 结果与来自疾病控制与预防中心(CDC WONDER)国家生命统计系统的过量死亡率数据之间的相关性。
设计、设置和参与者:这项回顾性的横断面研究包括 2013 年 1 月 1 日至 2020 年 12 月 31 日期间,由物质使用障碍(SUD)治疗医疗保健机构提交的 50 万份尿液样本进行 UDT。实时 UDT 数据来自 Millennium Health 专有国家数据库,过量死亡率数据来自疾病控制和预防中心(CDC WONDER)国家生命统计系统。使用液相色谱-串联质谱法对 5 个类别(可卡因、海洛因、甲基苯丙胺、合成阿片类药物和其他阿片类药物)的特定药物进行分析。参与者为年龄在 18 岁及以上、在 SUD 治疗机构提供尿液样本的成年人。
尿液药物检测。
主要结果是全国、州和县级 UDT 阳性率与过量死亡率之间的相关性。还使用单变量和多变量回归模型来评估州和县级过量死亡率与标准化 UDT 阳性率之间的关联。
在 2013 年至 2020 年间,从 SUD 治疗机构收集的 50 万份独特患者样本中,有 288534 份(57.7%)来自男性,研究人群的中位年龄为 34 岁(IQR,17-51 岁)。在全国范围内,合成阿片类药物和甲基苯丙胺与过量死亡率高度相关(Spearman ρ=0.96)。当合成阿片类药物共存时,甲基苯丙胺(ρ=0.98)、海洛因(ρ=0.78)、可卡因(ρ=0.94)和其他阿片类药物(ρ=0.83)也与过量死亡率高度相关。在没有合成阿片类药物的情况下,所有药物类别都高度相关(其他阿片类药物的 ρ=0.75,海洛因的 ρ=0.81,甲基苯丙胺的 ρ=0.88),可卡因除外(ρ=-0.37)。合成阿片类药物(ρ=0.77)和甲基苯丙胺(ρ=0.80)随着时间的推移具有最强的州级相关性,而其他阿片类药物的总阳性率(ρ=0.31)和在没有合成阿片类药物的情况下的阳性率(ρ=0.23)的相关性最低。在俄亥俄州,合成阿片类药物(ρ=0.71)、海洛因(ρ=0.69)和甲基苯丙胺(ρ=0.67)的县一级相关性最强。在州一级,合成阿片类药物的多变量发病率比(IRR)为 1.16(95%CI,1.14-1.19;P<0.001),在县一级,IRR 为 1.13(95%CI,1.09-1.17;P<0.001),这表明 UDT 阳性率每增加 1-SD,每月的过量死亡人数就会分别增加 16.2%和 12.8%。甲基苯丙胺(UDT 阳性率每增加 1-SD,死亡率增加 11.7%;IRR,1.12;95%CI,1.09-1.14;P<0.001)和可卡因(UDT 阳性率每增加 1-SD,死亡率增加 5.1%;IRR,1.05;95%CI,1.03-1.07;P<0.001)也与死亡率有显著的正相关,但效应大小小于合成阿片类药物(IRR,1.16)。
在这项研究中,UDT 结果与全国、州和县级的死亡率高度相关。这些发现表明,实时 UDT 监测可以帮助快速识别药物使用模式的变化,这可能为预防过量死亡而设计的有针对性的减少伤害策略提供信息。