Genesis Research, 111 River Street, Ste 1120, Hoboken, NJ, 07030, USA.
Eisai, Inc., 200 Metro Blvd., Nutley, NJ, 07110, USA.
BMC Geriatr. 2022 Jun 4;22(1):484. doi: 10.1186/s12877-022-03165-6.
Falls are the leading cause of injury-related death among older Americans. While some research has found that insomnia heightens falls, health care resource utilization (HCRU) and costs, the impact of insomnia treatments on fall risk, mortality, HCRU and costs in the elderly population, which could be of substantial interest to payers, has not been fully elucidated. This study evaluated the risk of falls and related consequences among adults ≥ 65 years of age treated with common prescription medications for insomnia compared with non-sleep disordered controls.
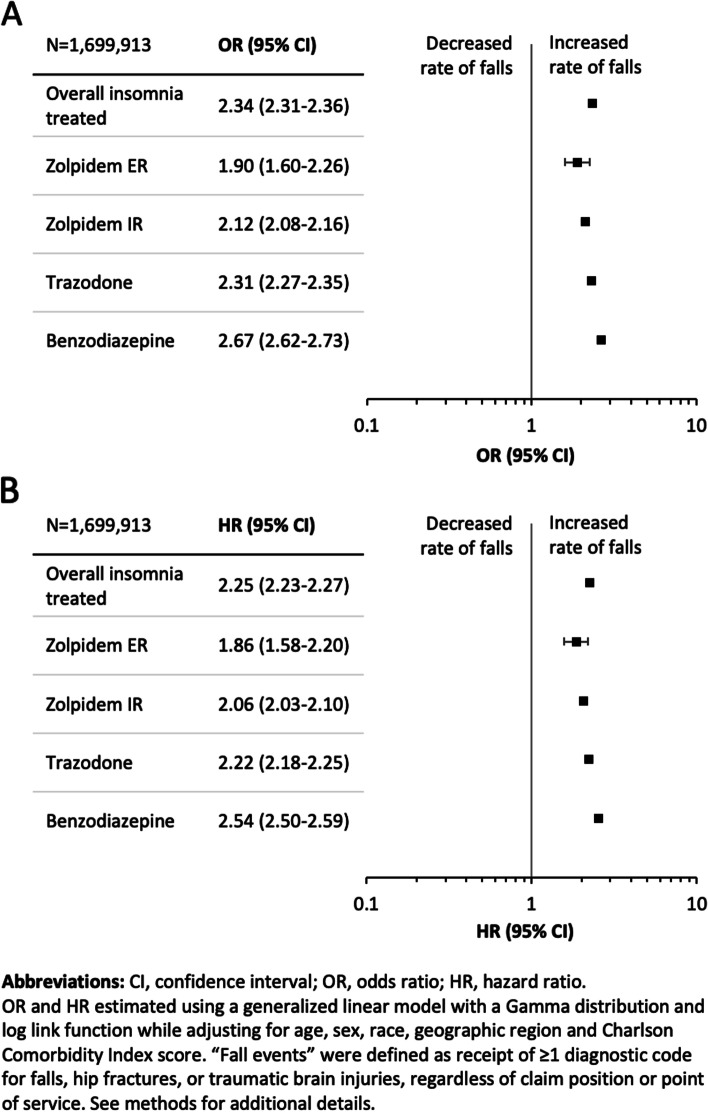
This was a retrospective cohort analysis of deidentified Medicare claims from January 2011 through December 2017. Medicare beneficiaries treated for insomnia receiving zolpidem extended-release, zolpidem immediate-release, trazodone, or benzodiazepines were matched with non-sleep disordered controls. The main outcomes were falls, mortality, healthcare resource utilization (HCRU), and medical costs during the 12 months following the earliest fill date for the insomnia medication of interest. Generalized linear models controlled for several key covariates, including age, race, sex, geographic region and Charlson Comorbidity Index score.
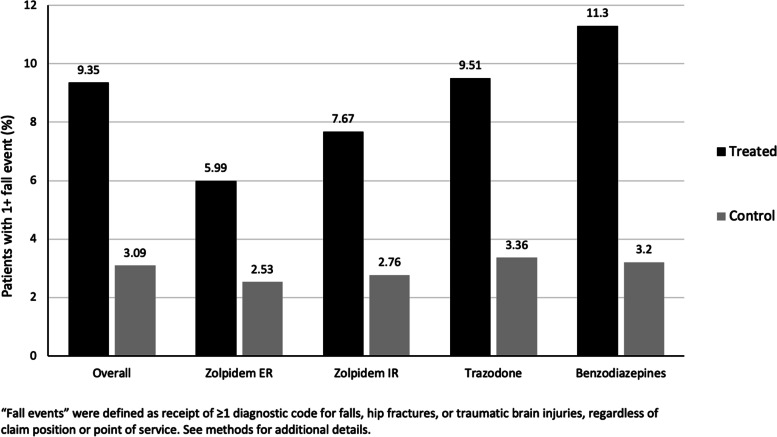
The study included 1,699,913 Medicare beneficiaries (59.9% female, mean age 75 years). Relative to controls, adjusted analyses showed that beneficiaries receiving insomnia medication experienced over twice as many falls (odds ratio [OR] = 2.34, 95% CI: 2.31-2.36). In adjusted analyses, patients receiving benzodiazepines or trazodone had the greatest risk. Crude all-cause mortality rates were 15-times as high for the insomnia-treated as controls. Compared with controls, beneficiaries receiving insomnia treatment demonstrated higher estimated adjusted mean number of inpatient, outpatient, and emergency department visits and longer length of inpatient stay. All-cause total adjusted mean costs were higher among insomnia treated patients ($967 vs $454).
Individuals receiving insomnia treatment had an increased risk of falls and mortality and higher HCRU and costs compared with matched beneficiaries without sleep disorders. Trazodone and benzodiazepines were associated with the greatest risk of falls. This analysis suggests that significant risks are associated with common, older generation insomnia medication treatments in the elderly. Nonetheless, these results should be interpreted with caution as the use of these medications may be indicative of underlying morbidity with potential for residual confounding.
在美国老年人中,跌倒导致的伤害相关死亡是主要原因。虽然一些研究发现失眠会增加跌倒的风险,但医疗保健资源利用(HCRU)和成本,失眠治疗对老年人跌倒风险、死亡率、HCRU 和成本的影响,这可能是支付者非常感兴趣的,尚未得到充分阐明。本研究评估了与非睡眠障碍对照相比,使用常见处方失眠药物治疗的≥65 岁成年人的跌倒风险及相关后果。
这是一项对 2011 年 1 月至 2017 年 12 月期间医疗保险索赔中未识别信息的回顾性队列分析。接受佐匹克隆延长释放剂、佐匹克隆即时释放剂、曲唑酮或苯二氮䓬类药物治疗失眠的医疗保险受益人与非睡眠障碍对照相匹配。主要结果是在感兴趣的失眠药物最早用药日期后 12 个月内发生的跌倒、死亡率、医疗资源利用(HCRU)和医疗费用。广义线性模型控制了几个关键协变量,包括年龄、种族、性别、地理位置和 Charlson 合并症指数评分。
该研究纳入了 1699913 名医疗保险受益人(59.9%为女性,平均年龄 75 岁)。与对照组相比,调整后的分析显示,接受失眠药物治疗的受益人的跌倒次数增加了两倍多(比值比[OR] = 2.34,95%CI:2.31-2.36)。在调整分析中,接受苯二氮䓬类或曲唑酮治疗的患者风险最大。失眠治疗组的全因死亡率是对照组的 15 倍。与对照组相比,接受失眠治疗的患者就诊的住院、门诊和急诊次数和住院时间均有所增加。全因总调整平均费用在失眠治疗患者中更高(967 美元对 454 美元)。
与无睡眠障碍的匹配受益相比,接受失眠治疗的个体发生跌倒和死亡的风险更高,HCRU 和费用更高。曲唑酮和苯二氮䓬类药物与跌倒风险增加有关。本分析表明,在老年人中,常用的第一代失眠药物治疗存在显著风险。尽管如此,由于这些药物的使用可能表明潜在的发病机制,并存在潜在的残余混杂因素,因此应谨慎解释这些结果。