Graduate Institute of Biomedical Informatics, College of Medical Science and Technology, Taipei Medical University, Taipei, Taiwan.
Clinical Big Data Research Center, Taipei Medical University Hospital, Taipei, Taiwan.
Prostate Cancer Prostatic Dis. 2023 Dec;26(4):722-729. doi: 10.1038/s41391-022-00555-0. Epub 2022 Jun 3.
The impact of gonadotropin-releasing hormone (GnRH) antagonist and agonist (GnRHa) treatment on cardiovascular disease (CVD) risk in prostate cancer (PCa) remains inconclusive due to conflicting findings. We compared the effects of GnRH antagonist and GnRHa treatments on CVD risk in patients with PCa and pre-existing CVD, in a Taiwan population-based database.
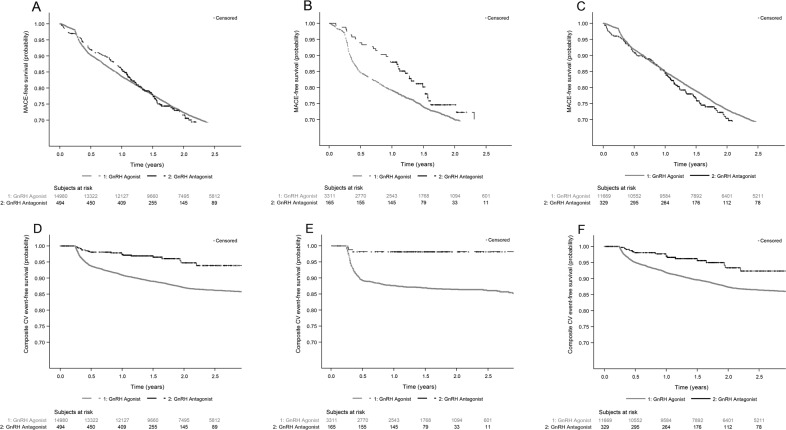
We assessed the risk of major adverse CV events (MACE: ischemic heart disease [IHD], stroke, congestive heart failure [CHF] or all cause deaths) and composite CV events (IHD, stroke, CHF or CV deaths) occurring ≥90 days after androgen deprivation therapy (ADT) initiation in patients with PCa after 90 days of treatment with either GnRH antagonist (degarelix; n = 499) or GnRHa (goserelin, leuprolide, triptorelin; n = 15,127). Patients identified with pre-existing CVD had received cardiac therapy for IHD, reported a stroke or CHF within a year before ADT initiation. Adjusted hazard ratios (aHR) and 95% confidence interval (CI) were obtained for MACE and composite CV events risk after adjusting for age, baseline status of diabetes, hypertension and treatments received.
All GnRH antagonist-treated patients showed lower risk of composite CV events than the GnRHa-treated patients. The lower composite CV events risk associated with GnRH antagonist was also observed in patients with metastasis at diagnosis (aHR 0.16; 95% CI, 0.04-0.38; p = 0.013) and those receiving ADT for more than six months (aHR 0.30; 95% CI, 0.16-0.54; p < 0.0001). In patients with pre-existing CVD, the MACE risk was 33% lower (aHR 0.67; 95% CI, 0.46-0.96; p = 0.0299) and composite CV events risk was 84% lower (aHR 0.16; 95% CI, 0.05-0.50; p = 0.0017) in GnRH antagonist-treated than the GnRHa-treated patients.
In patients with PCa and pre-existing CVD, GnRH antagonist use was associated with lower risks for composite CV events and MACE compared with GnRHa.
由于研究结果相互矛盾,促性腺激素释放激素(GnRH)拮抗剂和激动剂(GnRHa)治疗对前列腺癌(PCa)患者心血管疾病(CVD)风险的影响仍不确定。我们在台湾基于人群的数据库中比较了 GnRH 拮抗剂和 GnRHa 治疗对 PCa 合并预先存在的 CVD 患者 CVD 风险的影响。
我们评估了接受雄激素剥夺治疗(ADT)后 90 天内开始使用 GnRH 拮抗剂(地加瑞克;n=499)或 GnRHa(戈舍瑞林、亮丙瑞林、曲普瑞林;n=15127)治疗 90 天后,PCa 患者发生主要不良心血管事件(MACE:缺血性心脏病[IHD]、中风、充血性心力衰竭[CHF]或全因死亡)和复合心血管事件(IHD、中风、CHF 或心血管死亡)的风险。预先存在 CVD 的患者在 ADT 开始前一年内接受过 IHD 心脏治疗、报告过中风或 CHF。调整后的风险比(aHR)和 95%置信区间(CI)是通过调整年龄、基线糖尿病、高血压和接受治疗的情况后获得的。
所有 GnRH 拮抗剂治疗的患者发生复合心血管事件的风险均低于 GnRHa 治疗的患者。在诊断时转移的患者(aHR 0.16;95%CI,0.04-0.38;p=0.013)和接受 ADT 治疗超过 6 个月的患者(aHR 0.30;95%CI,0.16-0.54;p<0.0001)中,与 GnRH 拮抗剂相关的复合心血管事件风险较低。在预先存在 CVD 的患者中,MACE 风险降低 33%(aHR 0.67;95%CI,0.46-0.96;p=0.0299),复合心血管事件风险降低 84%(aHR 0.16;95%CI,0.05-0.50;p=0.0017)。
在患有 PCa 和预先存在 CVD 的患者中,与 GnRHa 相比,使用 GnRH 拮抗剂治疗与复合心血管事件和 MACE 风险降低相关。