Department of Radiation Oncology, The University of Texas MD Anderson Cancer Center, Houston.
Department of Sociology, Rice University, Houston, Texas.
JAMA Netw Open. 2022 Jun 1;5(6):e2215589. doi: 10.1001/jamanetworkopen.2022.15589.
Consolidative durvalumab after definitive chemoradiation for unresectable locally advanced non-small cell lung cancer (NSCLC) can significantly improve progression-free survival (PFS) and overall survival (OS), as shown in the PACIFIC trial. However, whether patients with driver variations derive equal benefit from this regimen remains unclear.
To compare outcomes of patients with locally advanced NSCLC with and without driver variations treated with the PACIFIC regimen.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study examined 104 patients with unresectable locally advanced NSCLC with mutational profiling treated at a tertiary cancer center with definitive chemoradiation and consolidative durvalumab from June 2017 through May 2020. Patients with recurrent disease or those receiving postoperative therapy were excluded. Outcomes were analyzed with Kaplan-Meier and multivariate regression analyses.
Patients were grouped according to the presence of non-KRAS driver variations (EGFR exon 19 deletion, EGFR exon 20 insertion, EGFR exon 21 mutation [L858R], ERBB2 exon 20 insertion, EML4-ALK fusion, MET exon 14 skipping, NTRK2 fusion), KRAS driver variations, or no driver variations.
The primary outcomes were PFS, OS, and second progression-free survival (PFS2) times.
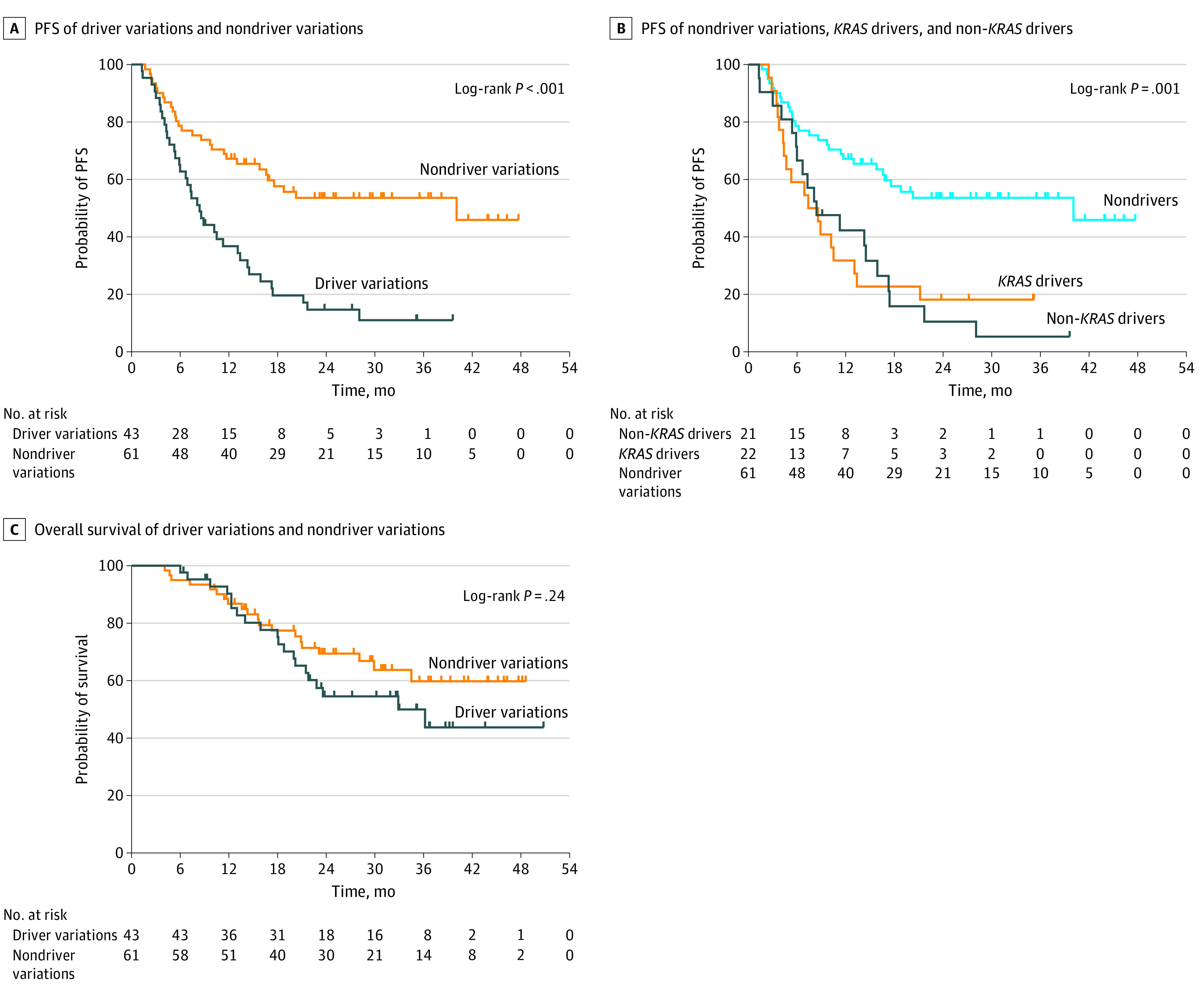
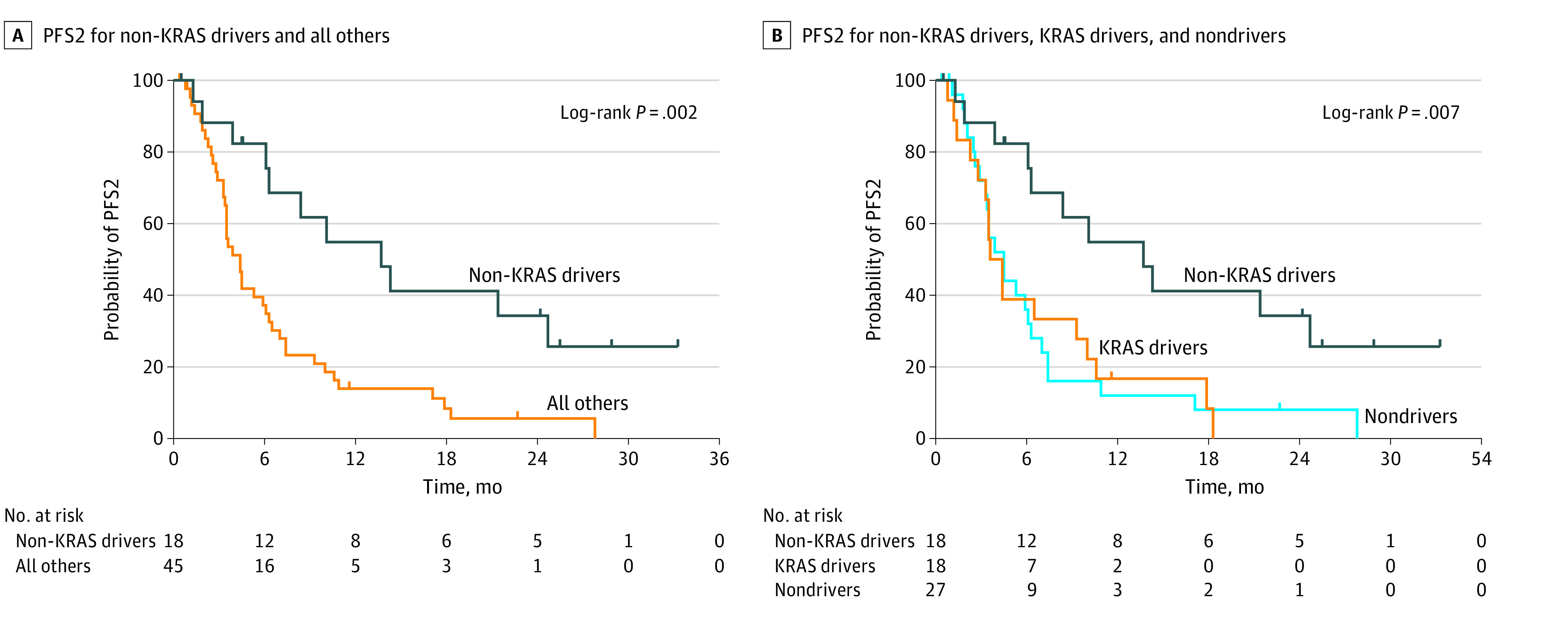
The 104 patients had a median (IQR) age of 65.1 (9.8) years, with 55 females (53%) and 85 former or current smokers (88%). There were 43 patients (41%) with driver variations with a median PFS time of 8.4 months vs 40.1 months for patients without driver variations (hazard ratio [HR], 2.75; 95% CI, 1.64-4.62; log-rank P < .001). Both patients with non-KRAS and KRAS driver variations had worse PFS. No difference in OS was found between patients with and without driver variations (log rank P = .24). Among the 63 patients who developed progressive disease, those with non-KRAS driver variations had a median PFS2 time of 13.7 months vs 4.4 months for all other patients (HR, 0.37; 95% CI, 0.21-0.64; log-rank P = .001). Rates of overall grade 2 toxic effects or higher did not differ by driver mutation status.
In this cohort study, driver variations in patients with unresectable locally advanced NSCLC were associated with significantly shorter PFS time after definitive chemoradiation and consolidative durvalumab. These findings suggest the need to consider additional or alternative treatment options to the PACIFIC regimen for patients with driver variations.
在不可切除的局部晚期非小细胞肺癌(NSCLC)患者中,在标准放化疗后进行巩固性 durvalumab 治疗可显著改善无进展生存期(PFS)和总生存期(OS),这在 PACIFIC 试验中得到了证实。然而,是否存在驱动基因突变的患者从这种治疗方案中获得同等获益仍不清楚。
比较局部晚期 NSCLC 患者在接受 PACIFIC 方案治疗时是否存在和不存在驱动基因突变的结局。
设计、地点和参与者:这项队列研究纳入了在一家三级癌症中心接受不可切除的局部晚期 NSCLC 治疗的 104 例经突变谱分析的患者,这些患者在 2017 年 6 月至 2020 年 5 月期间接受了标准放化疗和巩固性 durvalumab 治疗。排除了复发性疾病或接受术后治疗的患者。通过 Kaplan-Meier 和多变量回归分析评估了结局。
根据是否存在非 KRAS 驱动基因突变(EGFR 外显子 19 缺失、EGFR 外显子 20 插入、EGFR 外显子 21 突变[L858R]、ERBB2 外显子 20 插入、EML4-ALK 融合、MET 外显子 14 跳跃、NTRK2 融合)、KRAS 驱动基因突变或不存在驱动基因突变,将患者分为不同的组。
主要结局为 PFS、OS 和第二次无进展生存期(PFS2)。
这 104 例患者的中位(IQR)年龄为 65.1(9.8)岁,55 例女性(53%),85 例为既往或现吸烟者(88%)。43 例(41%)患者存在驱动基因突变,其中位 PFS 时间为 8.4 个月,而不存在驱动基因突变的患者中位 PFS 时间为 40.1 个月(HR,2.75;95%CI,1.64-4.62;log-rank P<0.001)。有非 KRAS 和 KRAS 驱动基因突变的患者 PFS 均更差。存在和不存在驱动基因突变的患者 OS 无差异(log-rank P=0.24)。在 63 例发生疾病进展的患者中,存在非 KRAS 驱动基因突变的患者 PFS2 时间的中位数为 13.7 个月,而其他患者的 PFS2 时间的中位数为 4.4 个月(HR,0.37;95%CI,0.21-0.64;log-rank P=0.001)。不同驱动基因突变状态患者的总体 2 级及以上毒性反应发生率无差异。
在这项队列研究中,不可切除的局部晚期 NSCLC 患者的驱动基因突变与标准放化疗和巩固性 durvalumab 治疗后的较短 PFS 时间显著相关。这些发现表明,对于存在驱动基因突变的患者,需要考虑 PACIFIC 方案以外的其他治疗选择。