School of Medicine, Oregon Health & Science University, Portland, Oregon, USA.
Department of Psychiatry, School of Medicine, University of Pittsburgh, Pittsburgh, Pennsylvania, USA.
Subst Abus. 2022;43(1):1251-1259. doi: 10.1080/08897077.2022.2074601.
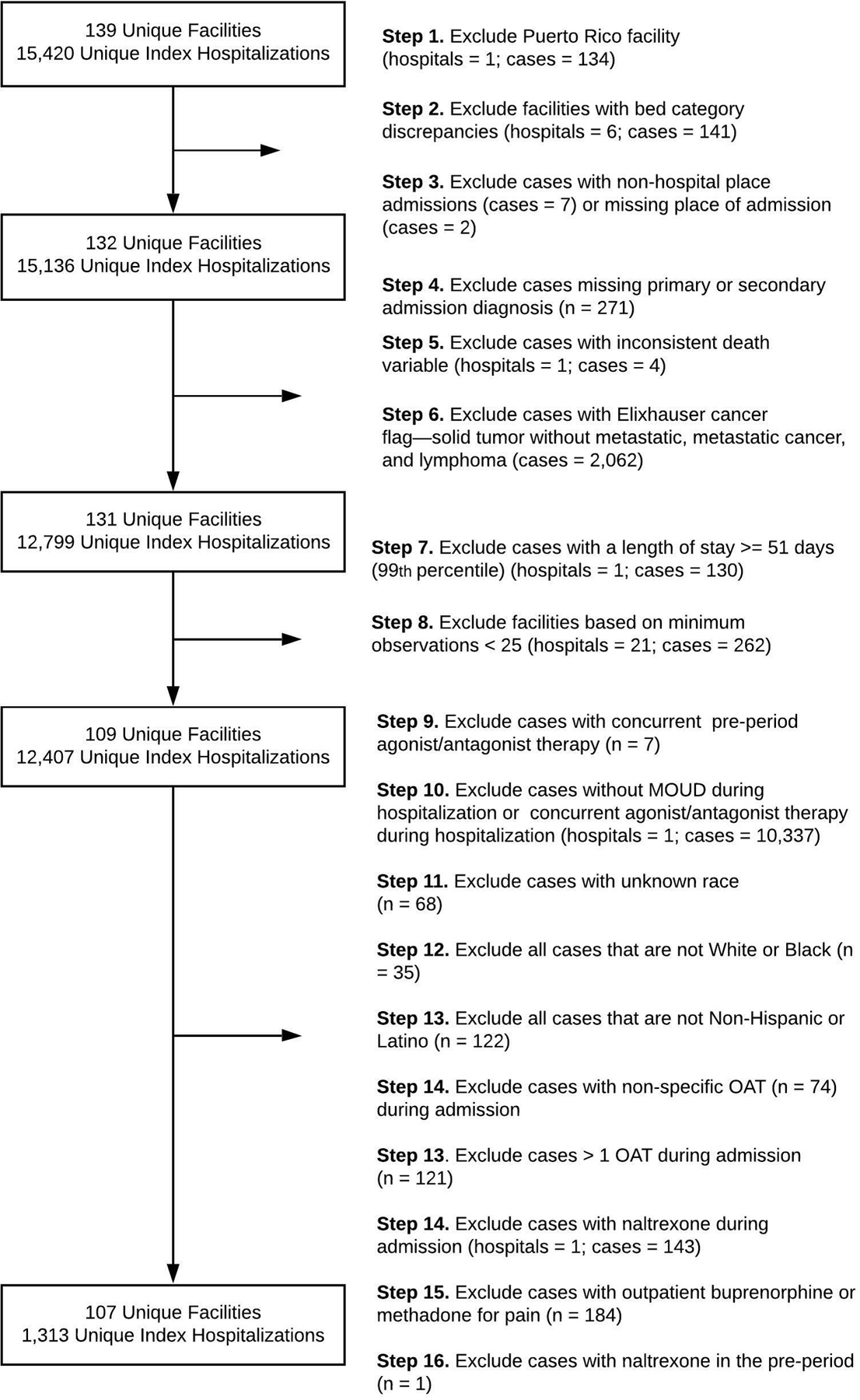
: As the drug-related overdose crisis and COVID-19 pandemic continue, communities need increased access to medications for opioid use disorder (MOUD) (i.e., buprenorphine and methadone). Disparities in the type of MOUD prescribed or administered by racial and ethnic categories are well described in the outpatient clinical environment. It is unknown, however, if these disparities persist when MOUD is provided in acute care hospitals. : This study assessed differences in the delivery of buprenorphine versus methadone during acute medical or surgical hospitalizations for veterans with opioid use disorder (OUD) by racial categories (Black Non-Hispanic or Latino vs. White Non-Hispanic or Latino). Data were obtained retrospectively from the Veterans Health Administration (VHA) for federal fiscal year 2017. We built logistic regression models, adjusted for individual and hospital-related covariates, and calculated the predicted probabilities of MOUD delivery by racial categories. : The study cohort ( = 1,313 unique patients; = 107 VHA hospitals) had a mean age of 57 (range 23 to 87 years), was predominantly male (96%), and composed entirely of Black (29%) or White (71%) patients. White patients were 11% more likely than Black patients to receive buprenorphine than methadone during hospitalization ( = 0.010; 95% CI: 2.7%, 20.0%). Among patients on MOUD prior to hospitalization, White patients were 21% more likely than Black patients to receive buprenorphine ( = 0.000; 95% CI: 9.8%, 31.5%). Among patients newly initiated on MOUD during hospitalization, there were no differences by racial categories. : We observed disparities in the delivery of buprenorphine versus methadone during hospitalization by racial categories. The observed differences in hospital-based MOUD delivery may be influenced by MOUD received prior to hospitalization within the racialized outpatient addiction treatment system. The VHA and health systems more broadly must address all aspects of racism that contribute to inequitable MOUD access throughout all clinical contexts.
: 在药物相关的过量用药危机和 COVID-19 大流行持续的情况下,社区需要增加获得阿片类药物使用障碍(MOUD)药物的途径(即丁丙诺啡和美沙酮)。在门诊临床环境中,按种族和族裔类别开出或管理的 MOUD 类型存在差异,这一点已经得到充分描述。然而,在急性护理医院提供 MOUD 时,这些差异是否仍然存在,则不得而知。: 本研究评估了在退伍军人阿片类药物使用障碍(OUD)的急性医疗或外科住院期间,按种族类别(黑种非西班牙裔或拉丁裔与白种非西班牙裔或拉丁裔),丁丙诺啡与美沙酮的使用差异。数据是从退伍军人健康管理局(VHA)获得的,时间为 2017 财年。我们建立了逻辑回归模型,调整了个体和医院相关的混杂因素,并按种族类别计算了 MOUD 给药的预测概率。: 研究队列( = 1313 名患者; = 107 家 VHA 医院)的平均年龄为 57 岁(范围 23 至 87 岁),主要为男性(96%),且全部由黑种人(29%)或白种人(71%)组成。与黑人患者相比,白人患者在住院期间接受丁丙诺啡而非美沙酮的可能性高 11%( = 0.010;95%CI:2.7%,20.0%)。在住院前接受 MOUD 治疗的患者中,白人患者接受丁丙诺啡的可能性比黑人患者高 21%( = 0.000;95%CI:9.8%,31.5%)。在住院期间新开始接受 MOUD 治疗的患者中,种族类别之间没有差异。: 我们观察到在住院期间,按种族类别提供丁丙诺啡与美沙酮之间存在差异。在基于医院的 MOUD 治疗方面观察到的差异可能受到在种族化的门诊成瘾治疗系统中住院前接受的 MOUD 治疗的影响。退伍军人健康管理局和更广泛的医疗系统必须解决导致所有临床环境中 MOUD 获得机会不平等的各个方面的种族主义。