Department of Medicine, Hematology/Oncology Division.
Department of Obstetrics and Gynecology.
J Clin Invest. 2022 Jul 15;132(14). doi: 10.1172/JCI158800.
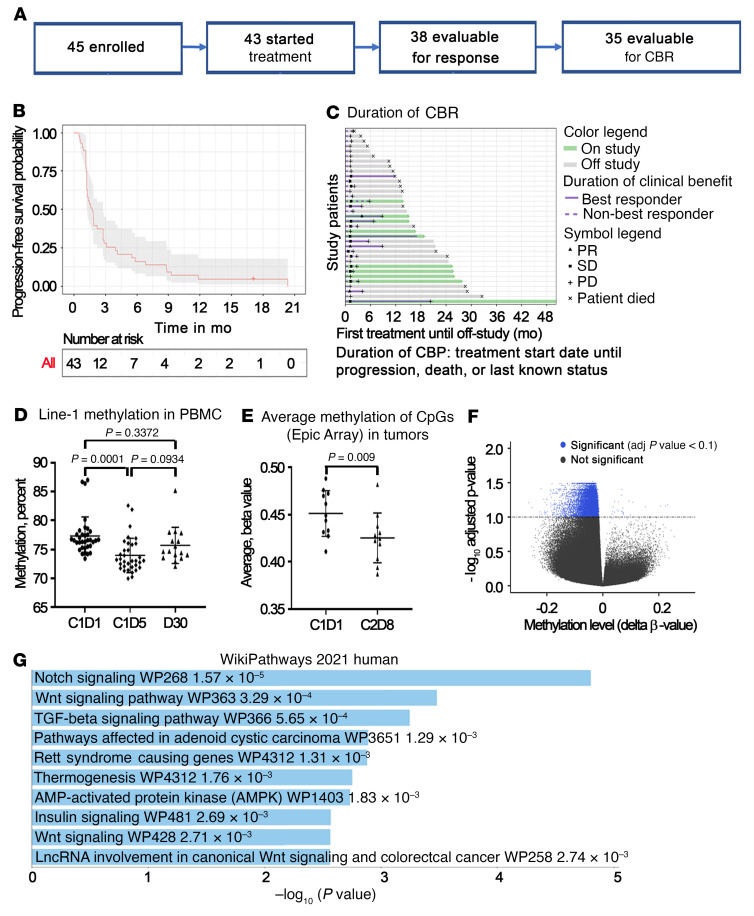
BackgroundImmune checkpoint inhibitors (ICIs) have modest activity in ovarian cancer (OC). To augment their activity, we used priming with the hypomethylating agent guadecitabine in a phase II study.MethodsEligible patients had platinum-resistant OC, normal organ function, measurable disease, and received up to 5 prior regimens. The treatment included guadecitabine (30 mg/m2) on days 1-4, and pembrolizumab (200 mg i.v.) on day 5, every 21 days. The primary endpoint was the response rate. Tumor biopsies, plasma, and PBMCs were obtained at baseline and after treatment.ResultsAmong 35 evaluable patients, 3 patients had partial responses (8.6%), and 8 (22.9%) patients had stable disease, resulting in a clinical benefit rate of 31.4% (95% CI: 16.9%-49.3%). The median duration of clinical benefit was 6.8 months. Long-interspersed element 1 (LINE1) was hypomethylated in post-treatment PBMCs, and methylomic and transcriptomic analyses showed activation of antitumor immunity in post-treatment biopsies. High-dimensional immune profiling of PBMCs showed a higher frequency of naive and/or central memory CD4+ T cells and of classical monocytes in patients with a durable clinical benefit or response (CBR). A higher baseline density of CD8+ T cells and CD20+ B cells and the presence of tertiary lymphoid structures in tumors were associated with a durable CBR.ConclusionEpigenetic priming using a hypomethylating agent with an ICI was feasible and resulted in a durable clinical benefit associated with immune responses in selected patients with recurrent OC.Trial registrationClinicalTrials.gov NCT02901899.FundingUS Army Medical Research and Material Command/Congressionally Directed Medical Research Programs (USAMRMC/CDMRP) grant W81XWH-17-0141; the Diana Princess of Wales Endowed Professorship and LCCTRAC funds from the Robert H. Lurie Comprehensive Cancer Center; Walter S. and Lucienne Driskill Immunotherapy Research funds; Astex Pharmaceuticals; Merck & Co.; National Cancer Institute (NCI), NIH grants CCSG P30 CA060553, CCSG P30 CA060553, and CA060553.
背景
免疫检查点抑制剂 (ICIs) 在卵巢癌 (OC) 中的活性有限。为了增强它们的活性,我们在一项 II 期研究中使用低甲基化剂 guadecitabine 进行初步治疗。
方法
合格的患者患有铂类耐药 OC、器官功能正常、可测量的疾病,并接受了多达 5 种先前的治疗方案。该治疗包括 guadecitabine(30mg/m2)在第 1-4 天,pembrolizumab(200mg 静脉注射)在第 5 天,每 21 天一次。主要终点是反应率。在基线和治疗后采集肿瘤活检、血浆和 PBMCs。
结果
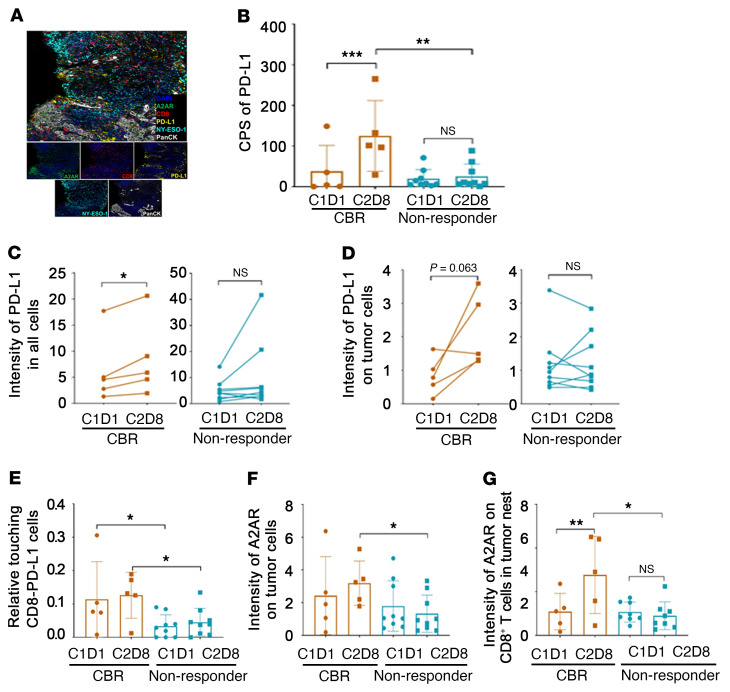
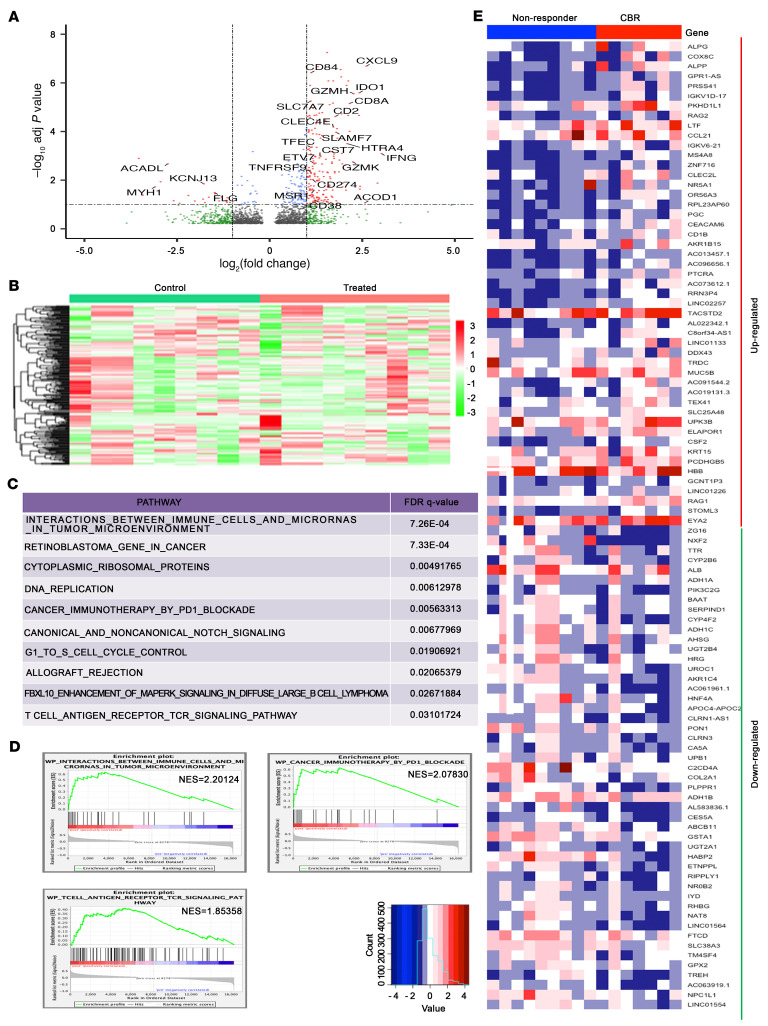
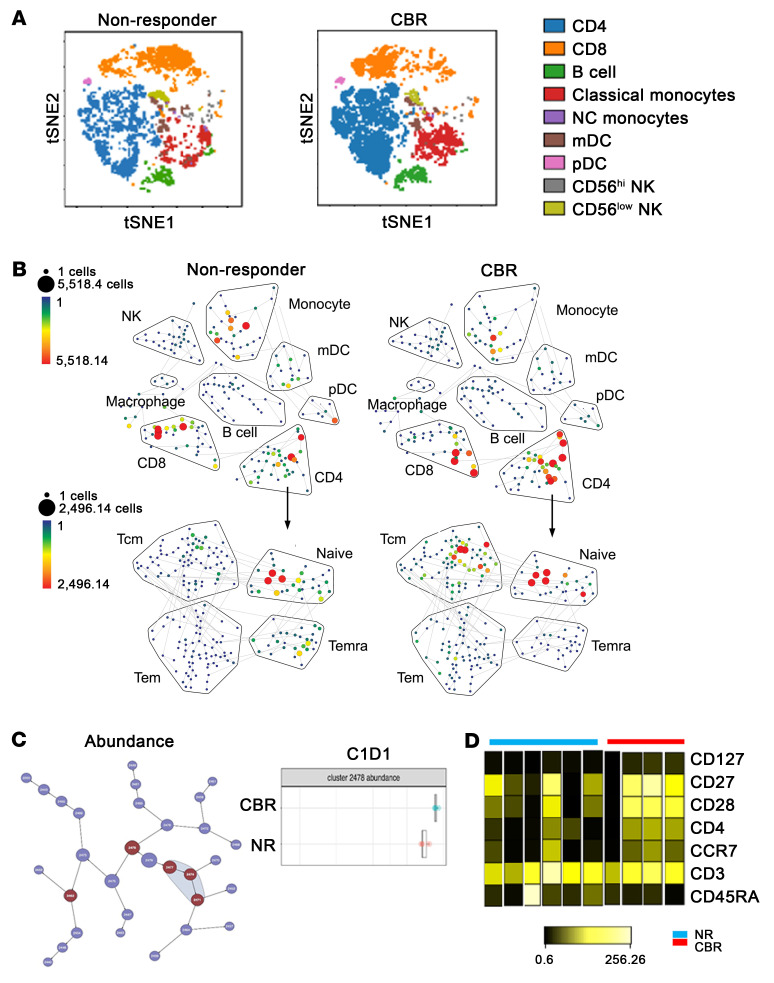
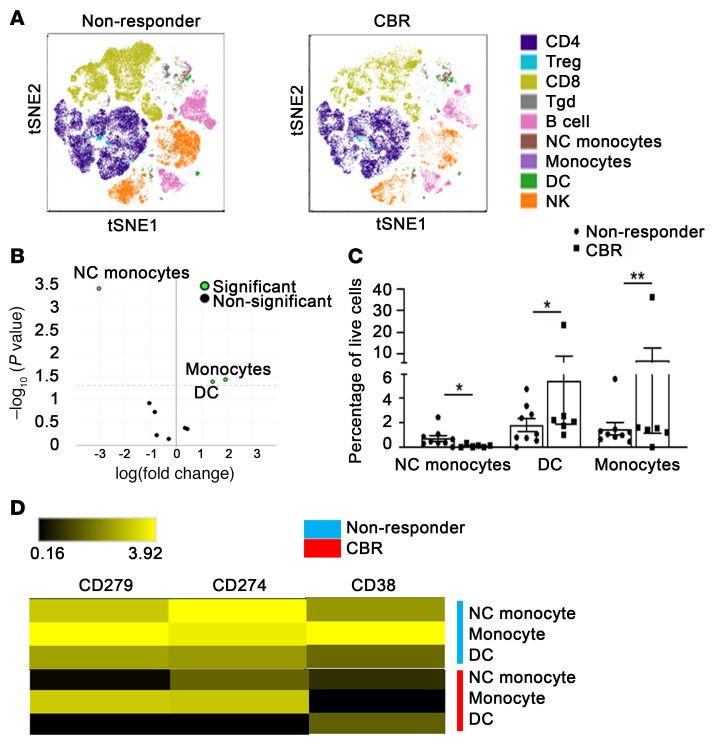
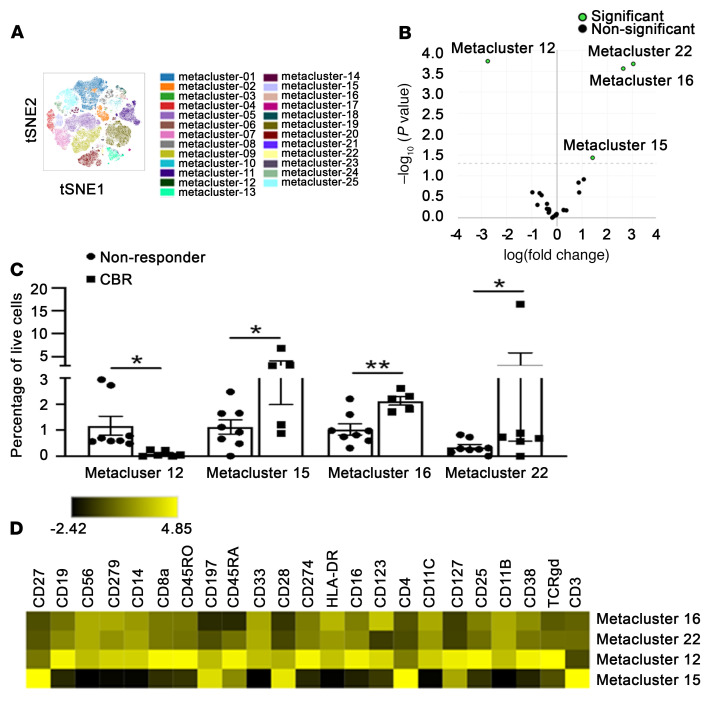
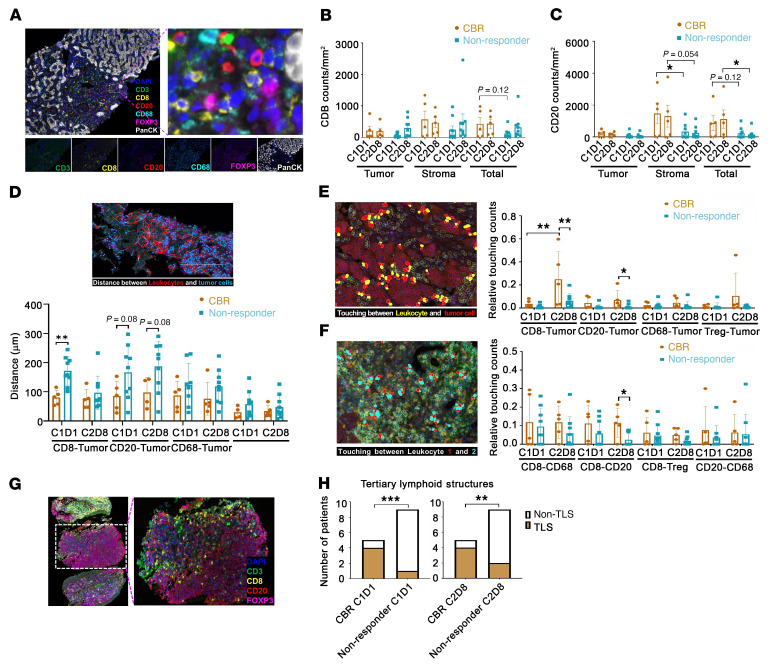
在 35 名可评估的患者中,3 名患者有部分缓解 (8.6%),8 名患者有稳定的疾病,临床获益率为 31.4% (95%CI:16.9%-49.3%)。临床获益的中位持续时间为 6.8 个月。治疗后 PBMCs 中的长散布元件 1 (LINE1) 被低甲基化,甲基组学和转录组学分析显示治疗后活检中抗肿瘤免疫的激活。PBMCs 的高维免疫分析显示,在具有持久临床获益或反应 (CBR) 的患者中,幼稚和/或中央记忆 CD4+T 细胞和经典单核细胞的频率更高。基线时 CD8+T 细胞和 CD20+B 细胞的密度较高以及肿瘤中存在三级淋巴结构与持久的 CBR 相关。
结论
使用低甲基化剂联合 ICI 进行表观遗传初步治疗是可行的,并在选定的复发性 OC 患者中产生了与免疫反应相关的持久临床获益。
试验注册
ClinicalTrials.gov NCT02901899。
资金来源
美国陆军军医研究与物资司令部/国会定向医学研究计划 (USAMRMC/CDMRP) 赠款 W81XWH-17-0141;戴安娜王妃基金会的 Diana Princess of Wales 特聘教授职位和 LCCTRAC 资金来自罗伯特·H·卢里综合癌症中心;Walter S. 和 Lucienne Driskill 免疫治疗研究基金;Astex 制药公司;默克公司;美国国立卫生研究院 (NCI),NIH 拨款 CCSG P30 CA060553、CCSG P30 CA060553 和 CA060553。