Husain-Syed Faeq, Reis Thiago, Kashani Kianoush, Ronco Claudio
Department of Internal Medicine II, University Hospital Giessen and Marburg, Justus-Liebig-University Giessen, Klinikstraße 33, 35392, Giessen, Germany.
Laboratory of Molecular Pharmacology, Faculty of Health Sciences, University of Brasília, Brasília, Distrito Federal, Brazil.
Pract Lab Med. 2022 Jun 2;31:e00283. doi: 10.1016/j.plabm.2022.e00283. eCollection 2022 Aug.
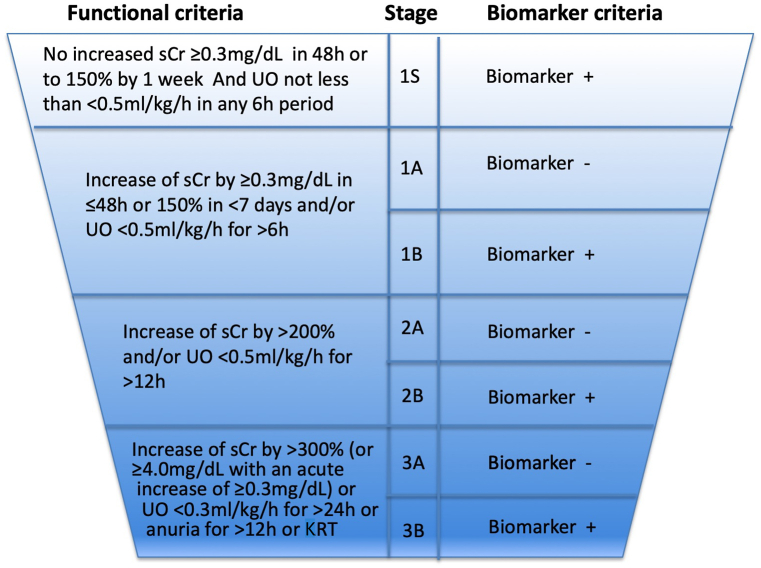
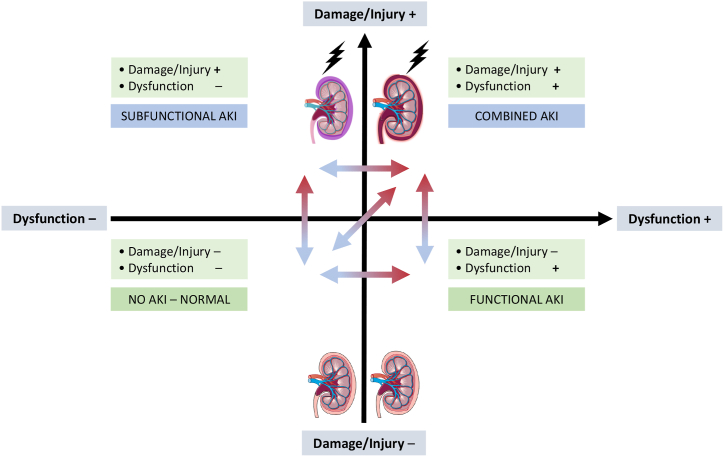
Recent advances have improved our understanding of the epidemiology and pathophysiology of acute kidney injury (AKI). So far, the Kidney Disease: Improving Global Outcome guidelines define and stratify kidney injury based on increases in serum creatinine level and/or decreases in urine output. Although the term AKI acknowledges the existence of cellular injury, its diagnosis is still only defined by the reduced excretory function of the kidney. New biomarkers that aid a better understanding of the relationship between acute tubular injury and kidney dysfunction have been identified, reflecting the advances in molecular biology. The expression of some of these novel biomarkers precedes changes in conventional biomarkers or can increase their predictive power. Therefore, they might enhance the clinical accuracy of the definition of AKI. This review summarizes the limitations of the current AKI classification and a panel of candidate biomarkers for augmenting AKI classification and recognition of AKI subphenotypes. We expect that the integration of appropriately selected biomarkers in routine clinical practice can improve AKI care.
近期的进展增进了我们对急性肾损伤(AKI)流行病学和病理生理学的理解。到目前为止,《改善全球肾脏病预后》指南基于血清肌酐水平升高和/或尿量减少来定义和分层肾损伤。尽管术语AKI承认细胞损伤的存在,但其诊断仍仅由肾脏排泄功能降低来定义。已鉴定出有助于更好理解急性肾小管损伤与肾功能障碍之间关系的新生物标志物,这反映了分子生物学的进展。其中一些新型生物标志物的表达先于传统生物标志物的变化,或者可以提高其预测能力。因此,它们可能会提高AKI定义的临床准确性。本综述总结了当前AKI分类的局限性以及一组用于增强AKI分类和识别AKI亚表型的候选生物标志物。我们期望在常规临床实践中适当选择生物标志物进行整合能够改善AKI的治疗。