Division of Allergology and clinical Immunology, Department of Pneumology and Allergology, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland.
Clinical Microbiology, Institute for Infectious Disease, University of Bern, Bern, Switzerland.
PLoS One. 2022 Jun 9;17(6):e0268780. doi: 10.1371/journal.pone.0268780. eCollection 2022.
Although mRNA-based vaccines against SARS-CoV-2 induce a robust immune response and prevent infections and hospitalizations, there are limited data on the antibody response in individuals with humoral immunodeficiency. The aim of this study was to evaluate the humoral immune response after two vaccine doses with BNT162b2 or mRNA-1273 in patients with humoral immunodeficiency disease.
This cross-sectional study assessed 39 individuals with hypogammaglobulinemia under immunoglobulin replacement therapy. IgG anti-SARS-CoV-2 spike protein antibodies (anti-S) were measured 4 weeks to 4 months after two doses of an mRNA vaccine against SARS-CoV-2. The proportion of patients, who developed a humoral immune response to the spike protein were evaluated and compared to 19 healthy controls.
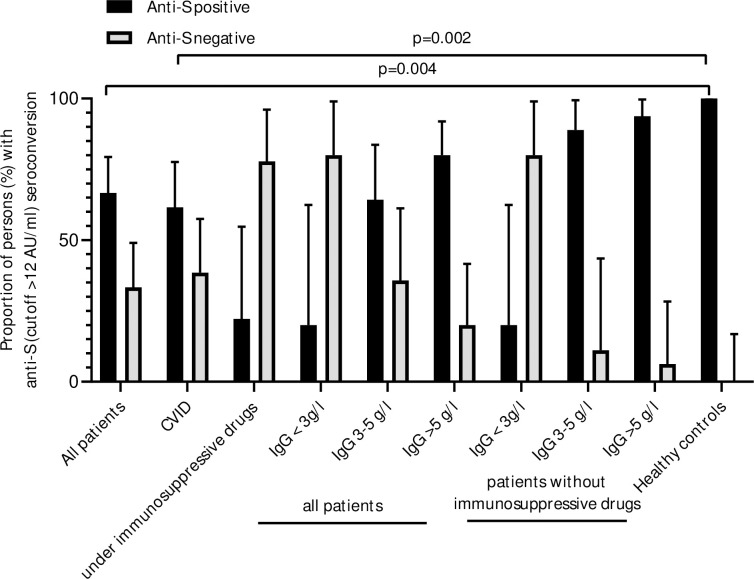
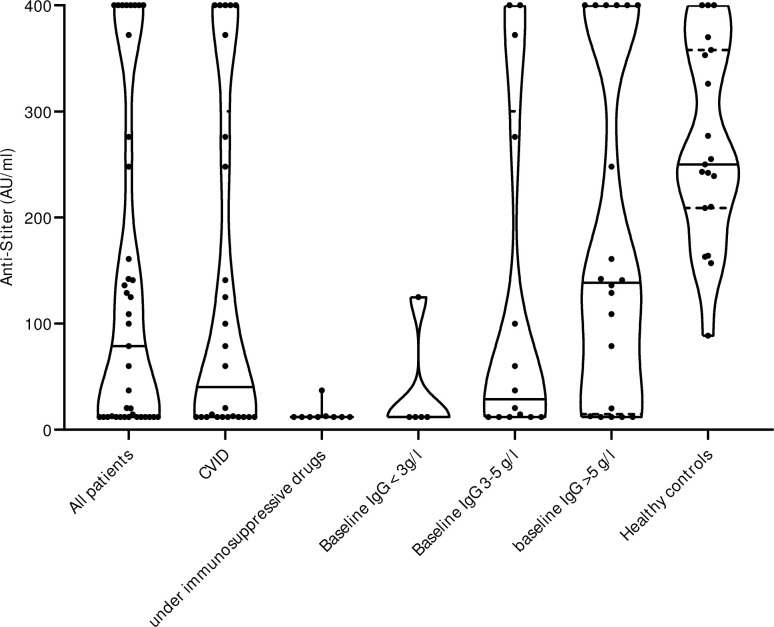
After vaccination with two vaccine doses, 26/39 patients (66.7%) with humoral immunodeficiency disease and all healthy controls developed anti-S. In subjects with baseline IgG <3 g/l, only 1/5 (20%) showed a humoral immune response. 10 out of 26 with CVID (38.5%) and 7/9 under immunosuppressive drugs (77.8%) developed no immune response (13 subjects with no response) compared to 0/19 in healthy controls. Subgroup analysis in patients without immunosuppressive drugs revealed lower anti-S in patients with moderate to severe humoral immunodeficiency disease: baseline IgG <3 g/l: 12.0 AU/ml (95%CI 12.0-125.0), baseline IgG 3-5 g/l: 99.9 AU/ml (95%CI 14.4-400.0), baseline IgG >5 g/l: 151.5 AU/ml (95%CI 109.0-400.0), healthy controls 250.0 AU/ml (95%CI 209.0-358.0), p = 0.007.
In most patients with mild to moderate humoral immunodeficiency we found only slightly lower anti-S antibodies compared with healthy controls after two vaccine doses with BNT162b2 and mRNA-1273. However, in patients with a decreased baseline IgG below 3 g/l and/or under immunosuppressive drugs, we found severely impaired humoral immune responses.
尽管基于 mRNA 的 SARS-CoV-2 疫苗可诱导强大的免疫应答并预防感染和住院,但关于体液免疫缺陷个体的抗体应答数据有限。本研究旨在评估接受 BNT162b2 或 mRNA-1273 两剂疫苗后体液免疫缺陷患者的体液免疫应答。
这项横断面研究评估了 39 名接受免疫球蛋白替代治疗的低丙种球蛋白血症患者。在接种 SARS-CoV-2 mRNA 疫苗后 4 周到 4 个月,测量 IgG 抗 SARS-CoV-2 刺突蛋白抗体(抗-S)。评估并比较了产生针对刺突蛋白的体液免疫应答的患者比例与 19 名健康对照者。
接种两剂疫苗后,39 名体液免疫缺陷患者中有 26 名(66.7%)和所有健康对照者均产生了抗-S。在基线 IgG<3 g/l 的患者中,仅有 1/5(20%)产生了体液免疫应答。26 名补体缺陷血管炎(CVID)患者中有 10 名(38.5%)和 9 名接受免疫抑制药物治疗的患者(77.8%)未产生免疫应答(13 名无应答者),而健康对照组中无应答者为 0/19。在无免疫抑制药物的患者亚组分析中,中度至重度体液免疫缺陷疾病患者的抗-S 水平较低:基线 IgG<3 g/l:12.0 AU/ml(95%CI 12.0-125.0),基线 IgG 3-5 g/l:99.9 AU/ml(95%CI 14.4-400.0),基线 IgG>5 g/l:151.5 AU/ml(95%CI 109.0-400.0),健康对照组 250.0 AU/ml(95%CI 209.0-358.0),p=0.007。
在接受 BNT162b2 和 mRNA-1273 两剂疫苗接种的大多数轻度至中度体液免疫缺陷患者中,与健康对照组相比,我们仅发现抗体水平略低。然而,在基线 IgG 低于 3 g/l 且/或接受免疫抑制药物治疗的患者中,我们发现严重受损的体液免疫应答。