Department of Medicine, Vagelos College of Physicians and Surgeons, Columbia University Irving Medical Center, New York, New York.
Department of Epidemiology, Mailman School of Public Health, Columbia University Irving Medical Center, New York, New York.
Cancer Prev Res (Phila). 2022 Oct 4;15(10):689-700. doi: 10.1158/1940-6207.CAPR-22-0013.
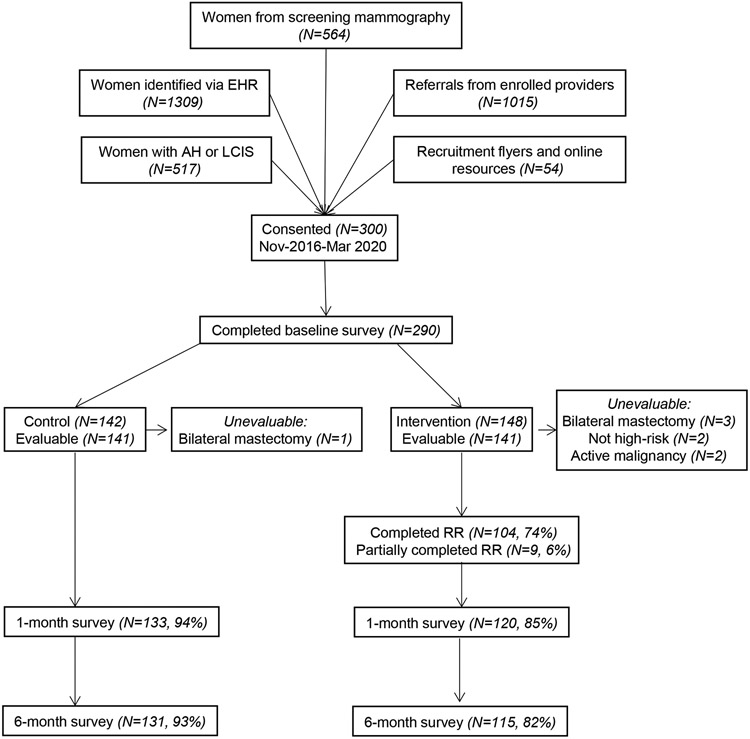
Significant underutilization of breast cancer chemoprevention remains, despite guidelines stating that physicians should recommend chemoprevention with antiestrogen therapy to high-risk women. We randomized women, ages 35 to 75 years, who met high-risk criteria for breast cancer, without a personal history of breast cancer or prior chemoprevention use, to standard educational materials alone or combined with a web-based decision aid. All healthcare providers, including primary care providers and breast specialists, were given access to a web-based decision support tool. The primary endpoint was chemoprevention uptake at 6 months. Secondary outcomes included decision antecedents (perceived breast cancer risk/worry, chemoprevention knowledge, self-efficacy) and decision quality (decision conflict, chemoprevention informed choice) based upon patient surveys administered at baseline, 1 and 6 months after randomization. Among 282 evaluable high-risk women enrolled from November 2016 to March 2020, mean age was 57 years (SD, 9.9) and mean 5-year invasive breast cancer risk was 2.98% (SD, 1.42). There was no significant difference in chemoprevention uptake at 6 months between the intervention and control groups (2.1% vs. 3.5%). Comparing the intervention and control arms at 1 month, there were significant differences among high-risk women in accurate breast cancer risk perceptions (56% vs. 39%, P = 0.017), adequate chemoprevention knowledge (49% vs. 27%, P < 0.001), mean decision conflict (34.0 vs. 47.0, P < 0.001), and informed choice (41% vs. 23%, P = 0.003). These differences were no longer significant at 6 months. Although our decision support tools did not result in a significant increase in chemoprevention uptake, we did observe improvements in decision antecedents and decision quality measures.
In this randomized controlled trial of decision support for 300 high-risk women and 50 healthcare providers, we did not observe a significant increase in chemoprevention uptake, which remained low at under 5%. However, these decision support tools may increase knowledge and informed choice about breast cancer chemoprevention.
未阐明的内容:尽管指南指出医生应建议具有乳腺癌高危因素且无乳腺癌病史或未使用过化学预防药物的女性使用抗雌激素疗法进行化学预防,但乳腺癌化学预防的使用率仍然很低。我们将年龄在 35 至 75 岁之间、具有乳腺癌高危因素、无乳腺癌病史或未使用过化学预防药物的女性随机分为仅接受标准教育材料组或在标准教育材料基础上联合基于网络的决策辅助组。所有医疗保健提供者,包括初级保健提供者和乳腺专家,都可以使用基于网络的决策支持工具。主要终点为 6 个月时化学预防的采用率。次要结局指标包括基于患者基线、随机分组后 1 个月和 6 个月时调查的决策前因(乳腺癌风险/担忧感知、化学预防知识、自我效能)和决策质量(决策冲突、化学预防知情选择)。2016 年 11 月至 2020 年 3 月期间共纳入 282 例可评估的高危女性,平均年龄为 57 岁(SD,9.9),5 年浸润性乳腺癌风险平均为 2.98%(SD,1.42)。干预组和对照组在 6 个月时的化学预防采用率无显著差异(2.1% vs. 3.5%)。与 1 个月时的干预组相比,高危女性在准确的乳腺癌风险认知(56% vs. 39%,P = 0.017)、足够的化学预防知识(49% vs. 27%,P < 0.001)、平均决策冲突(34.0 vs. 47.0,P < 0.001)和知情选择(41% vs. 23%,P = 0.003)方面存在显著差异。这些差异在 6 个月时不再显著。尽管我们的决策支持工具并未显著增加化学预防的采用率,但我们确实观察到决策前因和决策质量指标有所改善。
预防相关性:在这项针对 300 名高危女性和 50 名医疗保健提供者的决策支持随机对照试验中,我们未观察到化学预防采用率的显著增加,该比率仍低于 5%。然而,这些决策支持工具可能会增加对乳腺癌化学预防的认识和知情选择。