Department of Cardiology, Hospital Clínico UniversitarioVirgen de la Arrixaca, University of Murcia, Instituto Murciano de Investigación Biosanitaria (IMIB-Arrixaca), CIBERCV, Murcia, Spain.
Liverpool Centre for Cardiovascular Science, University of Liverpool, Liverpool Heart & Chest Hospital, Liverpool, UK.
Int J Clin Pract. 2022 May 26;2022:7325060. doi: 10.1155/2022/7325060. eCollection 2022.
Most evidence regarding anticoagulation and COVID-19 refers to the hospitalization setting, but the role of oral anticoagulation (OAC) before hospital admission has not been well explored. We compared clinical outcomes and short-term prognosis between patients with and without prior OAC therapy who were hospitalized for COVID-19.
Analysis of the whole cohort of the HOPE COVID-19 Registry which included patients discharged (deceased or alive) after hospital admission for COVID-19 in 9 countries. All-cause mortality was the primary endpoint. Study outcomes were compared after adjusting variables using propensity score matching (PSM) analyses.
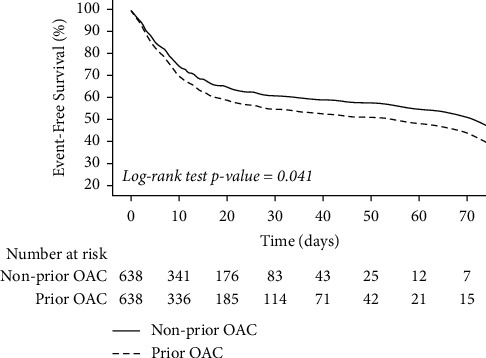
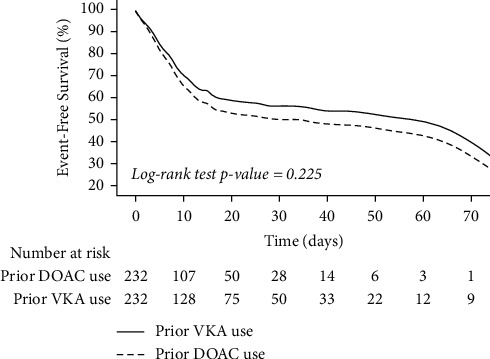
7698 patients were suitable for the present analysis (675 (8.8%) on OAC at admission: 427 (5.6%) on VKAs and 248 (3.2%) on DOACs). After PSM, 1276 patients were analyzed (638 with OAC; 638 without OAC), without significant differences regarding the risk of thromboembolic events (OR 1.11, 95% CI 0.59-2.08). The risk of clinically relevant bleeding (OR 3.04, 95% CI 1.92-4.83), as well as the risk of mortality (HR 1.22, 95% CI 1.01-1.47; log-rank value = 0.041), was significantly increased in previous OAC users. Amongst patients on prior OAC only, there were no differences in the risk of clinically relevant bleeding, thromboembolic events, or mortality when comparing previous VKA or DOAC users, after PSM.
Hospitalized COVID-19 patients on prior OAC therapy had a higher risk of mortality and worse clinical outcomes compared to patients without prior OAC therapy, even after adjusting for comorbidities using a PSM. There were no differences in clinical outcomes in patients previously taking VKAs or DOACs. This trial is registered with NCT04334291/EUPAS34399.
大多数关于抗凝和 COVID-19 的证据都涉及住院环境,但住院前口服抗凝治疗(OAC)的作用尚未得到充分探讨。我们比较了因 COVID-19 住院且有或无 OAC 治疗史的患者的临床结局和短期预后。
分析了在 9 个国家因 COVID-19 住院后出院(死亡或存活)的 HOPE COVID-19 注册研究的全队列。全因死亡率是主要终点。使用倾向评分匹配(PSM)分析调整变量后比较研究结果。
7698 例患者适合本分析(675 例入院时服用 OAC:427 例 VKA 和 248 例 DOAC)。PSM 后,分析了 1276 例患者(638 例服用 OAC,638 例未服用 OAC),血栓栓塞事件风险无显著差异(OR 1.11,95%CI 0.59-2.08)。临床相关出血风险(OR 3.04,95%CI 1.92-4.83)和死亡率风险(HR 1.22,95%CI 1.01-1.47;log-rank 值=0.041)显著增加。在仅服用 OAC 的患者中,经 PSM 后,比较 VKA 或 DOAC 前使用者,临床相关出血、血栓栓塞事件或死亡率风险无差异。
与未服用 OAC 治疗的 COVID-19 住院患者相比,服用 OAC 治疗的 COVID-19 住院患者的死亡率和临床结局更差,即使使用 PSM 调整合并症后也是如此。VKA 或 DOAC 前使用者的临床结局无差异。本试验在 NCT04334291/EUPAS34399 注册。