Department of Anaesthesia, Critical Care and Pain Medicine, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Massachusetts; Department of Anaesthesiology, Montefiore Medical Center, Albert Einstein College of Medicine, Bronx, New York.
Department of Anaesthesia, Critical Care and Pain Medicine, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Massachusetts.
Ann Thorac Surg. 2024 Jan;117(1):173-180. doi: 10.1016/j.athoracsur.2022.05.035. Epub 2022 Jun 8.
Reintubation after lung cancer resection is an important quality metric because of increased disability, mortality and cost. However, no validated predictive instrument is in use to reduce reintubation after lung resection. This study aimed to create and validate the PRediction Of REintubation After Lung cancer resection (PROREAL) score.
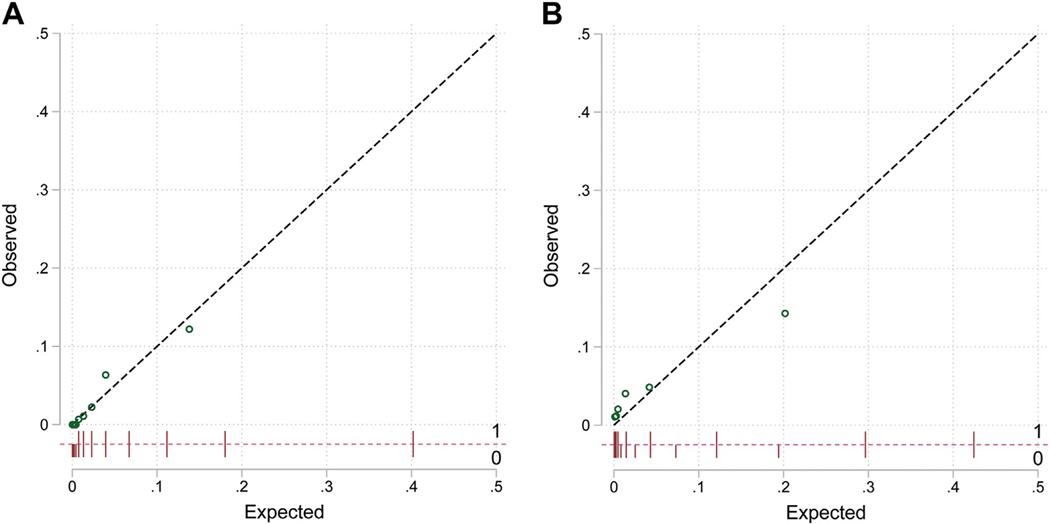
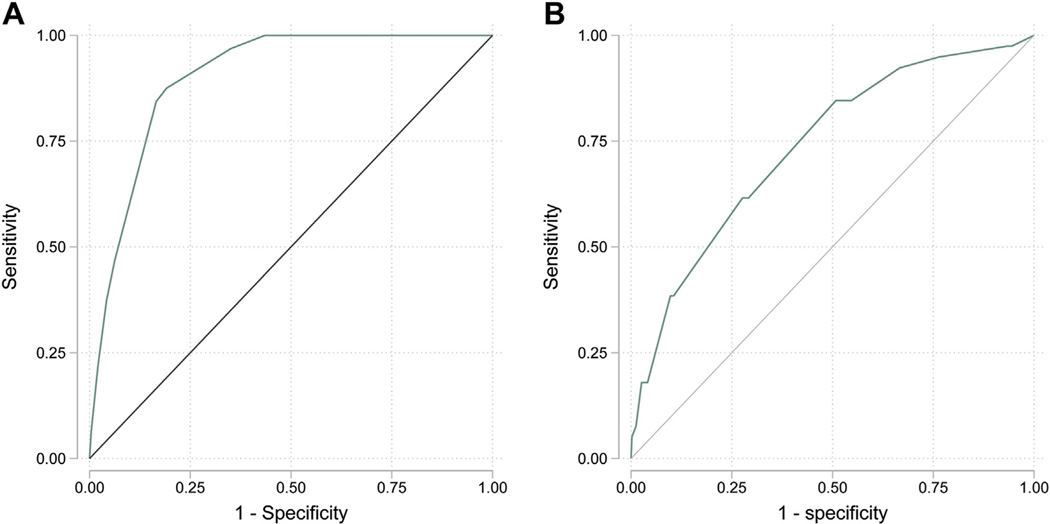
The study analyzed lung resection cases from 2 university hospitals. The primary end point was reintubation within 7 days after surgery. Predictors were selected through backward stepwise logistic regression and bootstrap resampling. The investigators used reclassification and receiver-operating characteristic (ROC) curve analyses to assess score performance and compare it with an established score for all surgical patients (Score for Prediction of Postoperative Respiratory Complications [SPORC]).
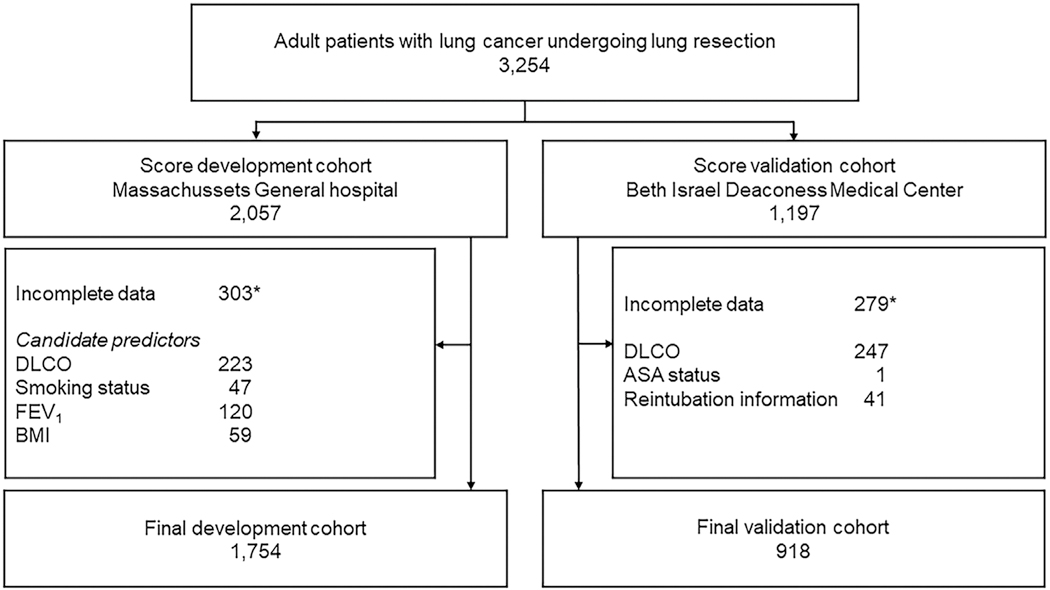
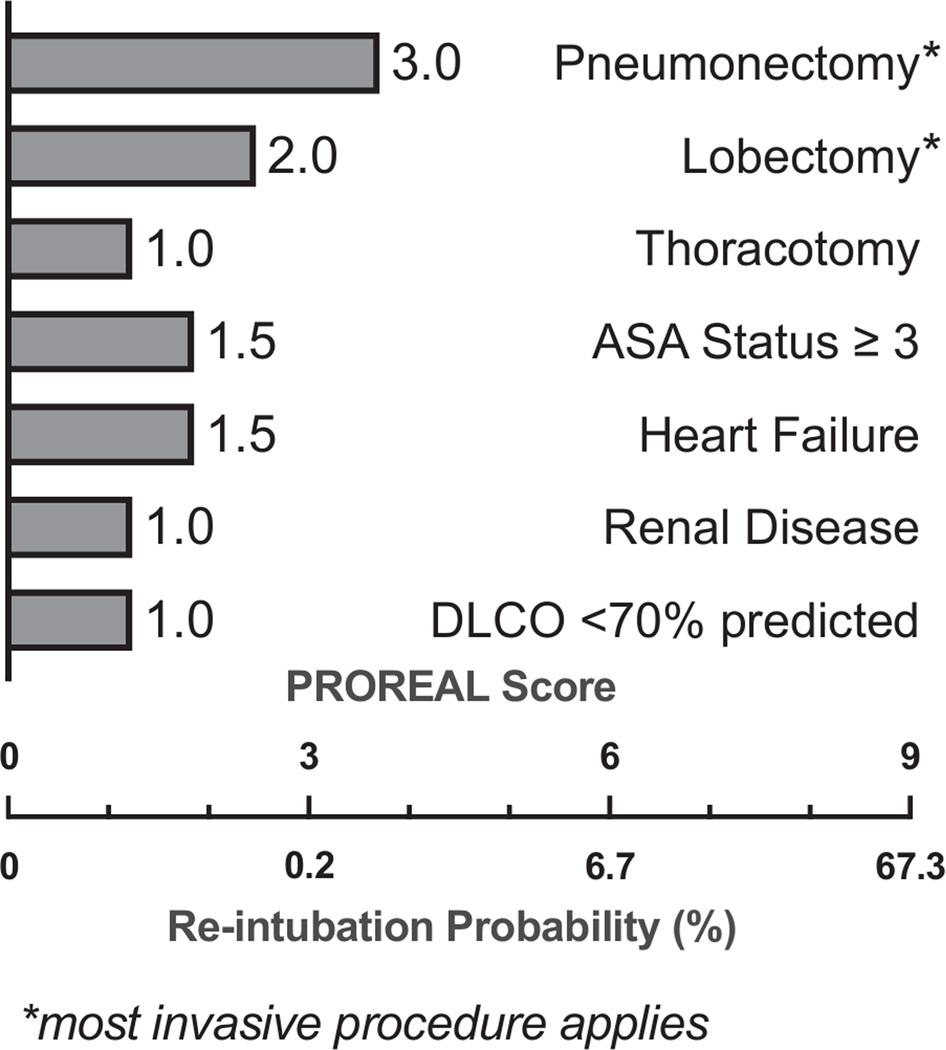
The study included 2672 patients who underwent resection for lung cancer (1754, development cohort; 918, validation cohort) between 2008 and 2020, of whom 71 (2.7%) were reintubated within 7 days after surgery. Identified score variables were surgical extent and approach, American Society of Anesthesiologists physical status, heart failure, renal disease, and diffusing capacity of the lung for carbon monoxide. The score achieved excellent discrimination in the development cohort (ROC AUC, 0.90; 95% CI, 0.87-0.94) and good discrimination in the validation cohort (ROC AUC, 0.74, 95% CI; 0.66-0.82), thus outperforming the SPORC in both cohorts (P < .001 and P = .018, respectively; validation cohort net reclassification improvement, 0.39; 95% CI, 0.18-0.60; P = .001). The score cutoff of ≥5 yielded a sensitivity of 88% (95% CI, 72-95) and a specificity of 81% (95% CI,79-83) in the development cohort.
A simple score (PROREAL) specific to lung cancer predicts postoperative reintubation more accurately than the nonspecific SPORC score. Operative candidates at risk may be identified for preventive intervention or alternative oncologic therapy.
肺癌切除术后再次插管是一个重要的质量指标,因为这会增加残疾、死亡率和成本。然而,目前尚无经过验证的预测工具可用于减少肺切除术后的再次插管。本研究旨在创建和验证预测肺癌切除术后再插管(PROREAL)评分。
该研究分析了来自 2 所大学医院的肺切除术病例。主要终点是术后 7 天内再次插管。通过向后逐步逻辑回归和自举重采样选择预测因子。研究人员使用重新分类和接收者操作特征(ROC)曲线分析来评估评分性能,并将其与所有手术患者的既定评分(术后呼吸并发症预测评分[SPORC])进行比较。
该研究纳入了 2008 年至 2020 年间接受肺癌切除术的 2672 例患者(发展队列 1754 例,验证队列 918 例),其中 71 例(2.7%)在术后 7 天内再次插管。确定的评分变量是手术范围和方法、美国麻醉医师协会身体状况、心力衰竭、肾脏疾病和一氧化碳弥散量。该评分在发展队列中具有出色的区分能力(ROC AUC,0.90;95%CI,0.87-0.94),在验证队列中具有良好的区分能力(ROC AUC,0.74,95%CI;0.66-0.82),因此在两个队列中的表现均优于 SPORC(P<0.001 和 P=0.018,分别;验证队列净重新分类改善,0.39;95%CI,0.18-0.60;P=0.001)。评分≥5 的截断值在发展队列中的敏感性为 88%(95%CI,72-95),特异性为 81%(95%CI,79-83)。
一种专门针对肺癌的简单评分(PROREAL)比非特异性 SPORC 评分更准确地预测术后再次插管。高危手术候选者可能需要进行预防性干预或替代肿瘤治疗。