Lin Xiaohui, Lin Minhua, Liu Maobai, Huang Weiying, Nie Xuekun, Chen Zichun, Zheng Bin
Department of Pharmacy, Ningde Municipal Hospital Affiliated to Ningde Normal University, Ningde, China.
Department of Pharmacy, Fujian Medical University Union Hospital, Fuzhou, China.
J Thorac Dis. 2022 May;14(5):1588-1597. doi: 10.21037/jtd-22-463.
The effect of empagliflozin on the cardiovascular outcome is consistent in heart failure with reduced ejection fraction (HFrEF) patients regardless of the presence or absence of diabetes. More evidence is needed regarding the cost-effectiveness of empagliflozin in HFrEF patients. This study sought to evaluate the economic outcomes of adding empagliflozin to the standard treatment for HFrEF patients from the perspective of the Chinese healthcare system, and thus to provide information for decision makers.
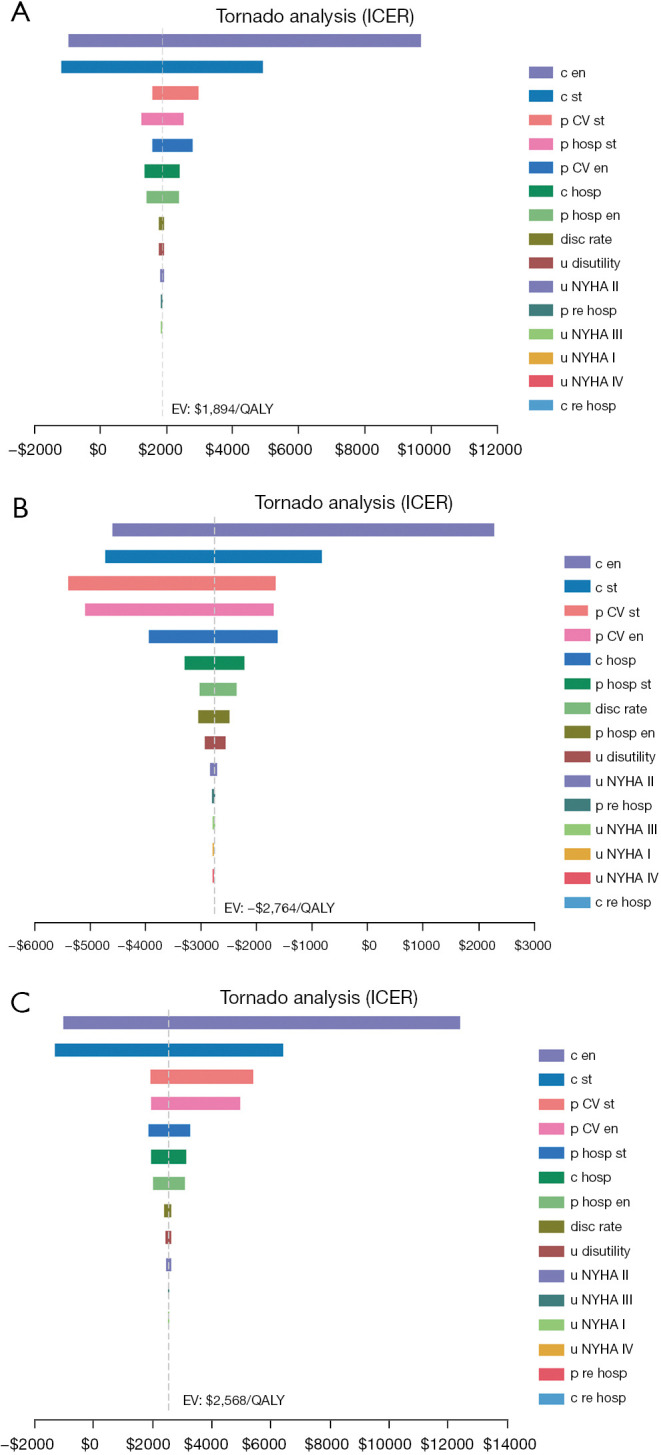
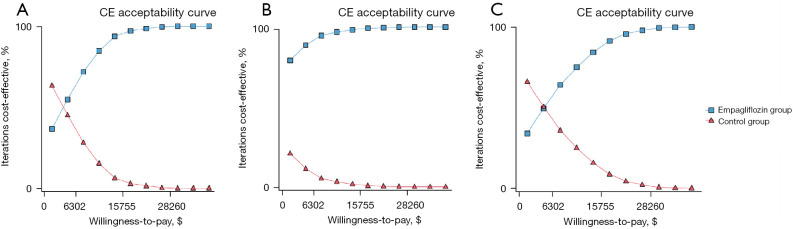
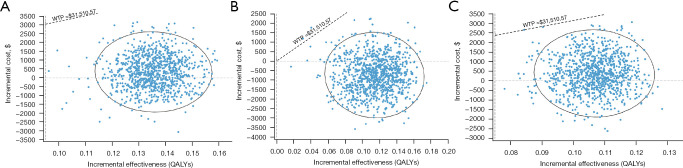
Based on the EMPEROR-Reduced clinical trial and other published literature data, the direct medical costs and quality-adjusted life years (QALYs) of patients with HFrEF over a 15-year study period were simulated by a Markov model, and the incremental cost-effectiveness ratio (ICER) was calculated. The price of empagliflozin referred to the data released by Menet, the hospitalization expenses and utility values were derived from published studies in China. A one-way sensitivity analysis and probabilistic sensitivity analysis were conducted to evaluate the robustness of the model.
The results of the cost-effectiveness analysis showed that the cost of the combination arm was $5,220.98, with a utility of 4.86 QALYs, and the cost of the standard arm was $4,873.96, with a utility of 4.68 QALYs, which equated to an ICER of $1,893.59 per QALY gained. The subgroup analysis showed that patients with HFrEF and diabetes in empagliflozin group had a higher QALY (4.62 4.35) and a lower cost ($5,213.28 $5,958.60) than standard group. The corresponding ICER for non-diabetic patients was $2,568.15 per QALY. Deterministic sensitivity analysis showed robust results. At the willingness-to-pay threshold of 3 times gross domestic product (GDP) per capita ($31,510.57), almost all of the scattered points in three scenarios were below the threshold line.
At a willingness-to-pay threshold of $31,510.57, adding empagliflozin to standard treatment is a very cost-effective option for HFrEF patients with or without diabetes in China.
无论是否患有糖尿病,恩格列净对射血分数降低的心力衰竭(HFrEF)患者的心血管结局影响是一致的。关于恩格列净在HFrEF患者中的成本效益,还需要更多证据。本研究旨在从中国医疗保健系统的角度评估在HFrEF患者的标准治疗中添加恩格列净的经济结局,从而为决策者提供信息。
基于EMPEROR-Reduced临床试验及其他已发表的文献数据,采用马尔可夫模型模拟HFrEF患者在15年研究期内的直接医疗成本和质量调整生命年(QALY),并计算增量成本效益比(ICER)。恩格列净的价格参考了美纳公布的数据,住院费用和效用值来自中国已发表的研究。进行了单向敏感性分析和概率敏感性分析以评估模型的稳健性。
成本效益分析结果显示,联合治疗组的成本为5220.98美元,效用为4.86个QALY,标准治疗组的成本为4873.96美元,效用为4.68个QALY,这相当于每获得1个QALY的ICER为1893.59美元。亚组分析显示,恩格列净组中患有HFrEF和糖尿病的患者比标准治疗组具有更高的QALY(4.62对4.35)和更低的成本(5213.28美元对5958.60美元)。非糖尿病患者的相应ICER为每QALY 2568.15美元。确定性敏感性分析显示结果稳健。在人均国内生产总值(GDP)3倍(31510.57美元)的支付意愿阈值下,三种情景下几乎所有散点均低于阈值线。
在支付意愿阈值为31510.57美元时,在中国,对于有或没有糖尿病的HFrEF患者,在标准治疗中添加恩格列净是一个非常具有成本效益的选择。