Gao Zhenzhen, Wu Na, Du Xuqin, Li Huiling, Mei Xue, Song Yuguo
Emergency Medicine Clinical Research Center, Beijing Chaoyang Hospital, Capital Medical University and Beijing Key Laboratory of Cardiopulmonary Cerebral Resuscitation, Beijing, People's Republic of China.
Department of Occupational Medicine and Clinical Toxicology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People's Republic of China.
Kidney Int Rep. 2022 Mar 18;7(6):1189-1197. doi: 10.1016/j.ekir.2022.03.009. eCollection 2022 Jun.
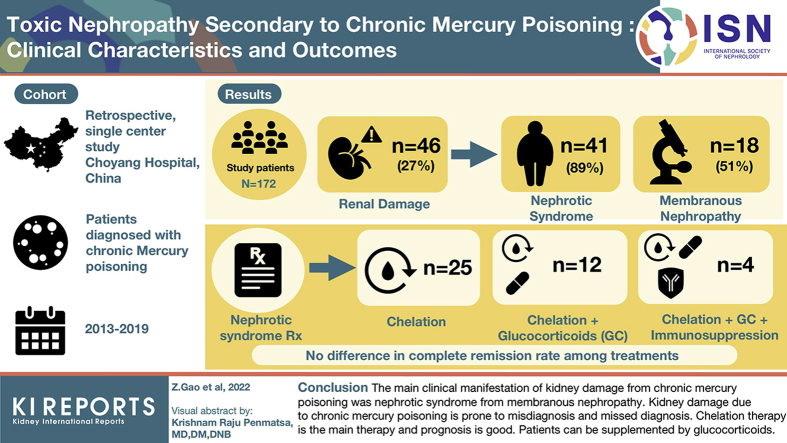
Kidney disease secondary to mercury poisoning has not been well documented and is often misdiagnosed and mistreated.
We performed a retrospective analysis of patients diagnosed with having mercury poisoning over a 6-year period between July 2013 and June 2019. Demographics, clinical measures, renal pathologic examinations, treatments, and outcomes were compared between patients with kidney disease and those without kidney disease.
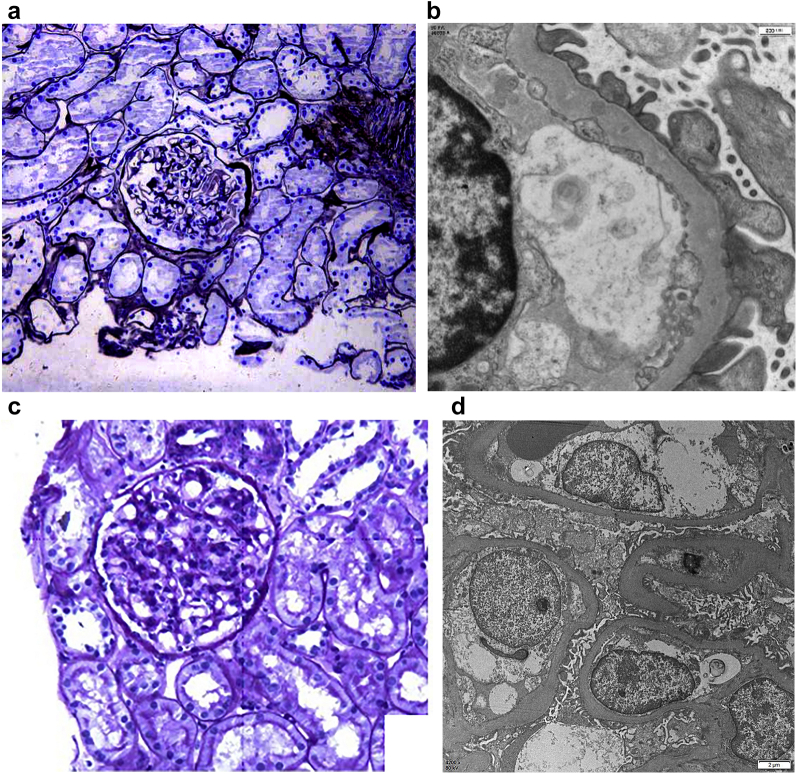
Of the 172 patients with mercury poisoning, 46 (26.74%) had renal damage. Among the 46 patients, 41 (89.13%) presented nephrotic syndrome, and 5 (10.87%) showed proteinuria alone. The pathologic abnormality associated with kidney disease caused by mercury poisoning was mainly membranous nephropathy (18 of 35 patients, 51.43%). Among 41 patients with nephrotic syndrome, 25 were treated with chelation therapy alone and 12 with mercury chelation therapy and glucocorticoids. The remaining 4 patients were treated with chelation therapy, glucocorticoids, and immunosuppressive therapies. The overall effective rate was 97.5% (40 patients). There was no significant difference in complete remission rate among the 3 treatment methods ( < 0.05).
The main clinical manifestation of kidney disease secondary to chronic mercury poisoning was nephrotic syndrome, which was reflected in pathologic examinations as membranous nephropathy. Kidney disease to chronic mercury poisoning is prone to misdiagnosis and missed diagnosis. Chelation therapy is the main treatment, and the prognosis is good. Patients with severe condition can be supplemented with glucocorticoid.
汞中毒继发的肾脏疾病尚未得到充分记录,常被误诊和误治。
我们对2013年7月至2019年6月期间6年内被诊断为汞中毒的患者进行了回顾性分析。比较了患有肾脏疾病和未患有肾脏疾病的患者的人口统计学、临床指标、肾脏病理检查、治疗方法及治疗结果。
172例汞中毒患者中,46例(26.74%)出现肾损害。在这46例患者中,41例(89.13%)表现为肾病综合征,5例(10.87%)仅表现为蛋白尿。汞中毒所致肾脏疾病相关的病理异常主要为膜性肾病(35例中的18例,51.43%)。41例肾病综合征患者中,25例仅接受螯合治疗,12例接受汞螯合治疗和糖皮质激素治疗。其余4例接受螯合治疗、糖皮质激素及免疫抑制治疗。总有效率为97.5%(40例患者)。3种治疗方法的完全缓解率差异无统计学意义(<0.05)。
慢性汞中毒继发肾脏疾病的主要临床表现为肾病综合征,病理检查表现为膜性肾病。慢性汞中毒所致肾脏疾病易误诊和漏诊。螯合治疗是主要治疗方法,预后良好。病情严重者可加用糖皮质激素。